
ACEP ID:
- My Account
- My CME
- Sign Out
ACEP ID:
Author: Sandra M. Schneider, MD, FACEP, Senior Vice President for Clinical Affairs, the American College of Emergency Physicians; Adjunct Professor of Emergency Medicine, University of Pittsburgh
The topic of ventilator shortages during a severe national pandemic or major disaster has been discussed and rehearsed during tabletop exercises. Triaging of ventilators should occur only when the hospital, region, or nation is operating in crisis mode. Ideally, planning for such an event should take place in advance and should involve hospital personnel, the ethics committee, and members of the public. Preplanning mitigates the enormity of the decision that must be made by an individual physician caring for a patient.
As ventilators become scarce, attempts should be made to increase the number of devices available. Hospitals should create a communication system or dashboard to locate available units within their institution and in cooperation with other facilities in their region and state. Ventilators used on animals are identical to those for humans, so veterinarian options should be explored.
It is possible to ventilate more than one patient (ie, up to four patients) with a single ventilator. Although the Society of Critical Care Medicine opposes this option in the “Consensus Statement on Multiple Patients Per Ventilator,” other agencies offer this option when conditions are dire, including the US Public Health Service Commissioned Corps in “Optimizing Ventilator Use During the COVID-19 Pandemic.”
During the height of the COVID-19 pandemic, other countries faced a ventilator shortage and created guidelines for intubation based on projected patient survival from COVID-19. These guidelines consider the patient's age and comorbidities as well as the survival data.
Perhaps the best plan on ventilator allocation open to the public is New York’s ventilator allocation guidelines.
Other documents that discuss ventilator allocation over a larger geographic region include:
It is difficult, if not impossible, to have all the necessary facts at hand when making decisions on intubation and ventilator use. Most scoring systems are based on the sequential organ failure assessment (SOFA) score, which is unavailable in the emergency department. The New York guidelines suggest that some patients should be considered for exclusion from ventilator support and, in times of ventilator scarcity, would not be candidates for intubation (see the ventilator allocation guidelines for further details).
Exclusion criteria include:
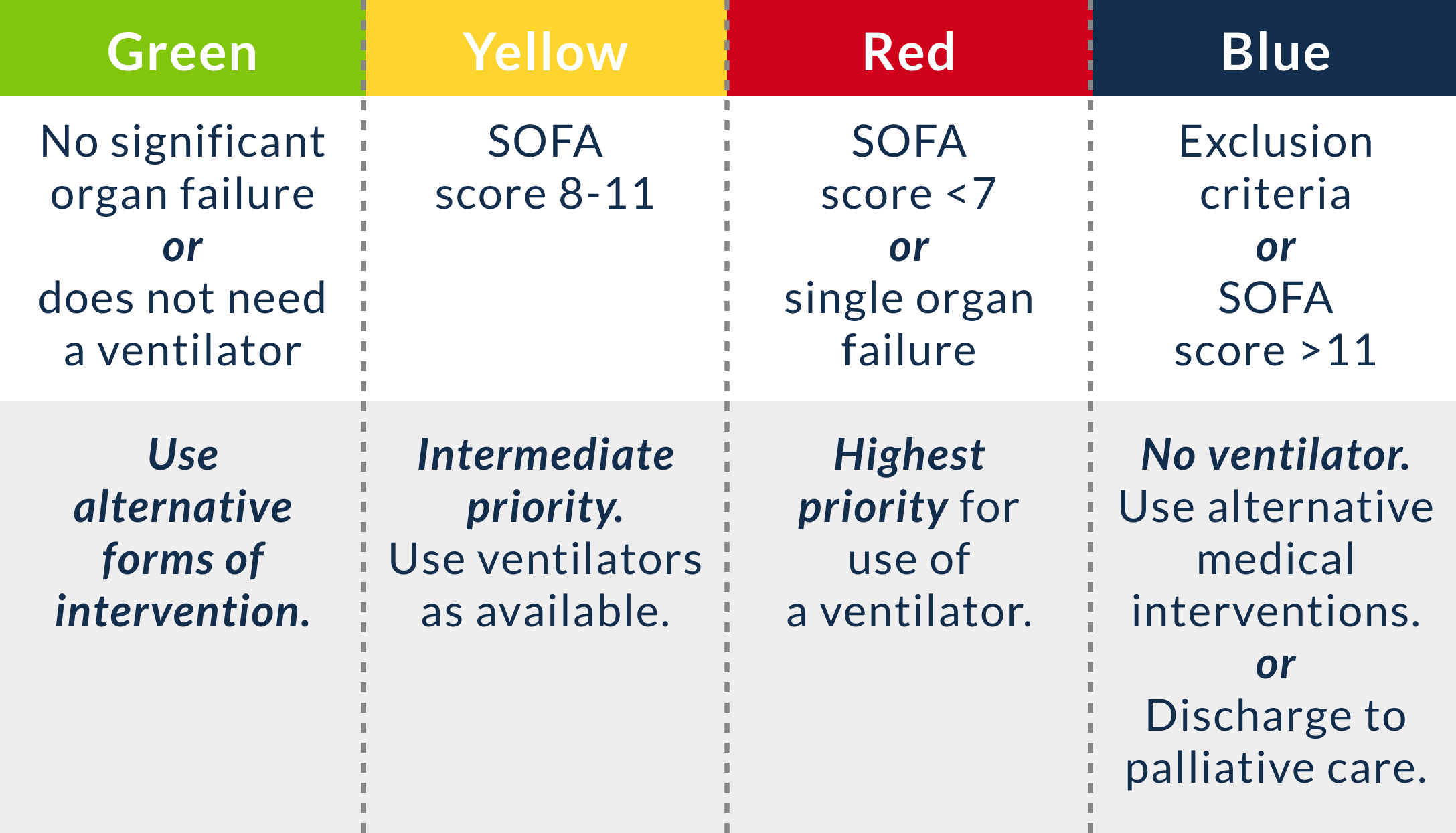
Presuming there is enough time for information gathering, the New York guidelines also rely on the SOFA score, which assigns a color code of priority for ventilators (Figure 12.2):
For more information, refer to MDCALC’s SOFA score calculator.
Figure 12.2 Color-coded SOFA scoring system
Patients are reassessed at 48 hours and periodically over time; the guidelines have additional information for decisions at these points in time.
Other plans exist or are modified from the New York guidelines. It is essential that a plan be in place to assist the physicians who must make these difficult decisions in the emergency department and ICU.