Overview
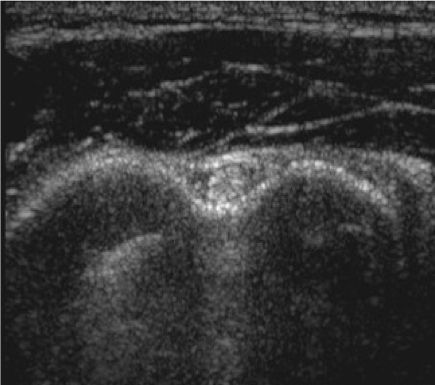
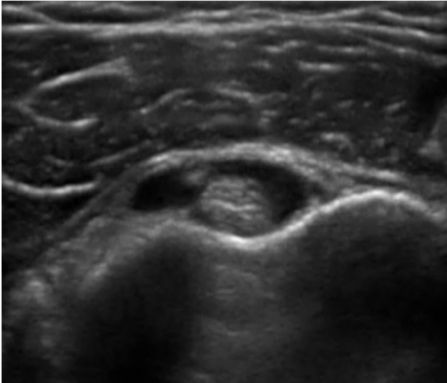
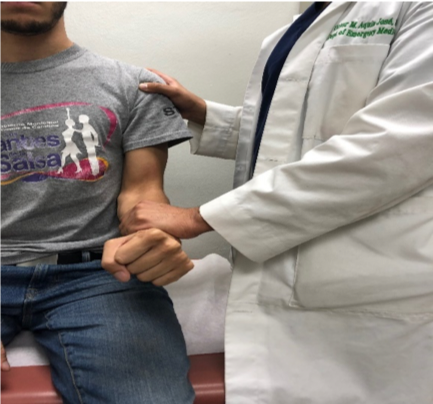
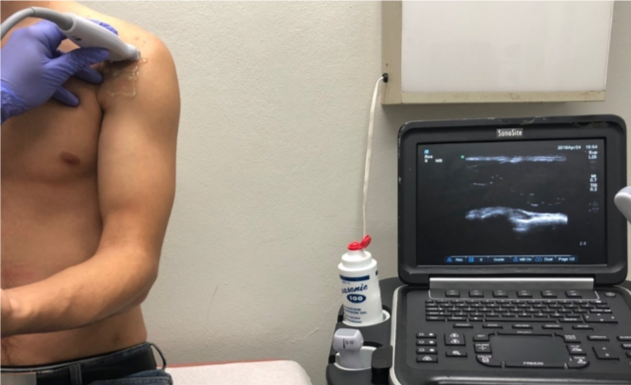
Bicipital tendinitis is a condition caused by inflammation of the long head of the biceps muscle’s tendon. It’s commonly caused by sudden overuse of the muscle and rotator cuff pathology such as muscle or tendon tears, chronic impingement, multidirectional shoulder instability, calcifications, and deconditioning. Signs in physical examination correlating with bicipital tendinitis are pain at the bicipital groove and a positive provocative test such as Speed’s test and Yergason’s test, although studies have shown that their sensitivity might be poor.1