Have the patient sit facing away from you, with the affected arm at the side in a neutral position.
Figure 1
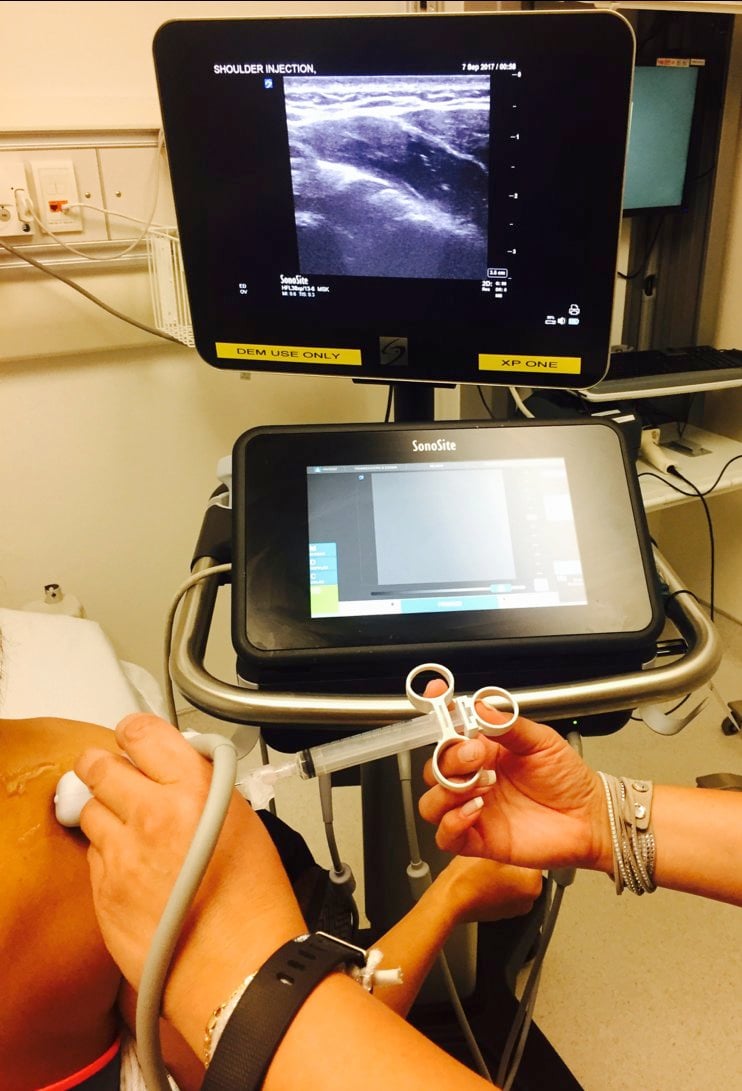
Place the ultrasound machine in front of the patient on the affected side.
Disinfect the skin.
Place a sterile cover over the ultrasound probe and apply sterile gel.
Place the probe in a transverse orientation over the infraspinatus and posterior glenohumeral joint, along the axis of the spine of the scapula and just caudal to the acromion.
Figure 2
Identify the humeral head, glenoid labrum, infraspinatus tendon, and joint capsule.
- Normally, the humeral head is located in the glenoid fossa. Figure 3
- In an anterior shoulder dislocation, the humeral head is located in the far field (deep to the probe). Figure 4
Place a skin wheal with local anesthetic lateral to the probe with a small-bore needle.
Enter the skin 1 cm lateral to the probe and advance the needle from the lateral to medial direction.
Keep the probe in a transverse orientation and use an in-plane technique.
Enter the shoulder joint between the posterior glenoid labrum and the insertion of the infraspinatus tendon on the hyperechoic (bright) humeral head.
Once in the joint, aspirate to make sure the needle is not in a vessel. It is common to get a flash of blood when you’re in the joint. 8
Inject 15-20 mL of local anesthetic into the joint space, visualizing the needle at all times. If it cannot be visualized, stop the procedure.
The patient should start to experience pain relief within 10 minutes. The duration of the block should be 3 to 8 hours, depending on the anesthetic used.