Procedure & Administration
Place the patient supine with the affected leg/hip slightly abducted, if possible.
Pull any adipose tissue out of the inguinal crease with tape.
Place the US machine on the opposite side of the bed.
Locate the femoral nerve using a high-frequency linear probe.
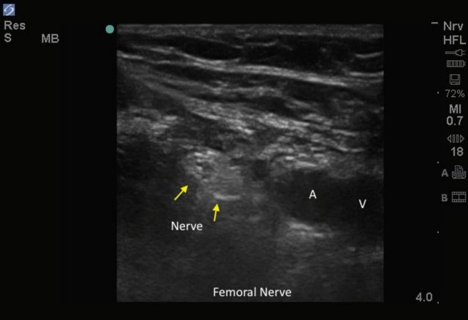
Remember “NAVEL”: Nerve, Artery, Vein, Empty, Lymphatics moving from lateral to medial.
Figure 1
Place the US probe parallel to the inguinal crease
- The femoral vein (more medial) will be more compressible than the artery (more lateral).
- Color Doppler mode can also be used to better identify the vessels.
The nerve lies immediately lateral to pulsating artery
- If there appears to be two arteries move proximally until you see one large femoral artery
Once the nerve has been found, place a local skin wheal of anesthetic.
Prep the area using a skin disinfectant and antiseptic.
Place a sterile probe cover over the US probe.
With a needle attached to the anesthetic syringe, enter the skin 1 cm lateral to the probe, with the needle bevel up
- Entry of the needle should generally be at a 45-degree angle but will depend upon the depth of the fascia iliaca.
To best visualize the needle tip, keep the US probe in a transverse orientation, and use an in-plane technique.
Advance the needle slowly, and aim toward the hyperechoic fascia iliaca, which typically overlies the femoral nerve.
- You may feel two “pops” as you penetrate the fascia lata and fascia iliaca.
Once deep to the fascia iliaca, aspirate back to make sure the needle is not in a vessel.
Stay at least 1 cm lateral to the femoral nerve to avoid accidental puncture of a vessel.
Once below the fascia iliaca, slowly inject 3 to 5 ml of anesthetic to confirm location.
- As the anesthetic is injected, it will have a hypoechoic (dark) appearance, and the anterior edge of the fascia iliaca will bulge forward (indicates filling of the fascia iliaca compartment).
- The patient may experience pressure at the injection site but if they experience sharp electric pain, stop injecting, and remove needle 1-2 mm before continuing with infiltration
After confirming location within the fascia iliaca, continue to inject 10 to 20 ml of anesthetic in small 3- to 5-mL aliquots.
- Anesthetic surrounding the nerve distally may give a “donut-like” appearance on US.
VISUALIZE THE INJECTION OF THE ANESTHETIC AT ALL TIMES.
- If you cannot visualize the injection, stop the procedure.
- The patient should start to experience pain relief within 15 minutes and full blockade after 30 minutes.