

Pain Management and Chest Tube Thoracostomy
Chest tube thoracostomy is standard of care for many emergent and non-emergent conditions in the emergency department (ED), including pneumothorax, hemothorax, and empyema. Despite its clinical utility, tube thoracostomy is painful and poorly tolerated, commonly requiring opioids during and after the procedure.1 Beyond the acute setting, chest tubes can be a source of chronic pain, causing difficulty to treat intercostal neuralgia.2
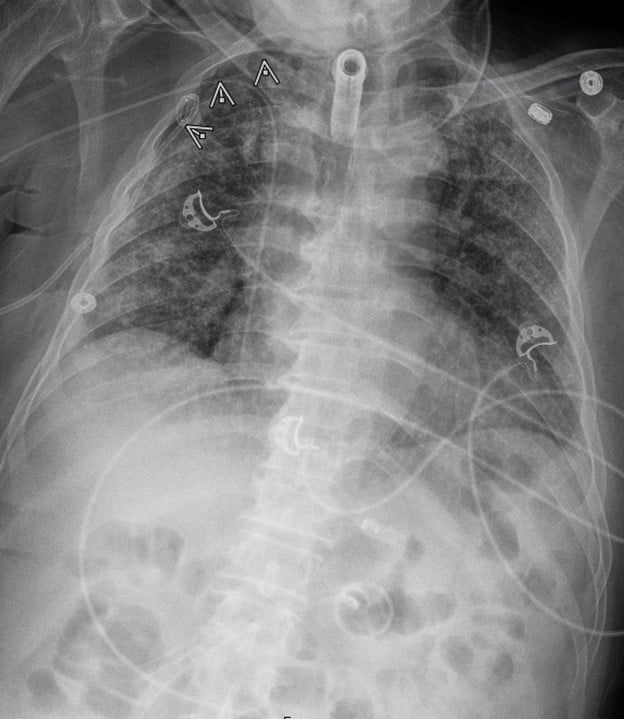
Target directed pain management therapies to the causal nerve, bone, or tendon provide a unique way to provide analgesia while decreasing the need for opiate consumption. The Serratus Anterior Plane Block (SAPB) is a commonly used regional block that was developed as a safer alternative to the thoracic paravertebral and neuro-axial thoracic epidural.3 It provides hemi-thoracic analgesia by blocking the thoracodorsal, long-thoracic, and intercostal nerves from T2-T9. Herein, we describe the use of a SAPB for non-emergent thoracostomy for the treatment of a spontaneous pneumothorax. The patient was a 62 year old male who presented to the ED with worsening dyspnea and was found to have a moderate-sized right-sided spontaneous pneumothorax without midline shift. The decision was made to pursue the placement of a pig-tail catheter and admit for observation. Prior to pig-tail placement, a SAPB was performed to optimize intra-procedure and postoperative pain control. The SAP block was performed by placing a linear transducer in the coronal plane in the mid-axillary line, starting at the clavicle and moving caudal to the fourth rib space, wherein the serratus anterior can be identified superficial to the ribs and deep to the latissimus dorsi. A mixture of 15 mls of Bupivacaine 0.5% and 15 mls of saline for a total volume of 30 cc was injected into the fascial plane located between the serratus anterior and latissimus dorsi. This was well below the toxic dose of 2-2.5mg/kg.4 The patient developed analgesia extending from approximately T2/T3 to T8, and the patient tolerated pigtail catheter placement at the fourth intercostal space. The patient required no additional pain medication after the initial placement and had good pain control after being evaluated two hours and six hours after the block was completed. The chest x-ray is provided below.
A recent meta-analysis of randomized control trials demonstrates that a SAPB block after thoracic surgery with reduced postoperative opioid consumption and nausea and vomiting compared to standard of care.5 Outside of post-surgical pain, the SAP block has been shown to be an effective and durable means of treating pain associated with rib fractures in the ED.6 Notably, the SAP block also offers longer lasting analgesia when compared to local infiltration, with up to 750-840 minutes per Blanco’s initial study which used 0.125% levobupivacaine, the S-enantiomer of bupivacaine, which can help reduce the need for opiates that may suppress respiratory drive and subsequently increase risk of aspiration, atelectasis, pneumonia and delirium (especially in older populations). Given that it is relatively easy and quick to perform with minimal side effects, the SAP block represents a safe, effective alternative to standard of care in the treatment of thoracic pain in the acute setting.

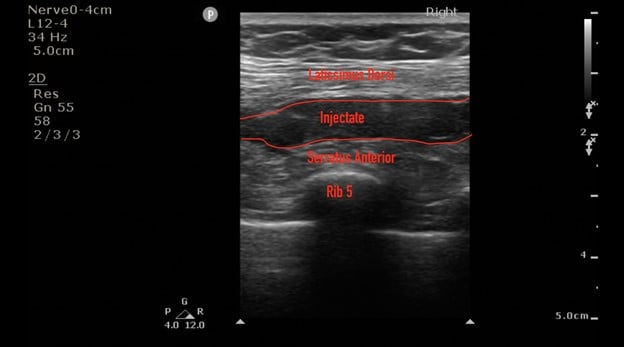
Ultrasound images courtesy of Christopher Moore, MD
References
- Luketich JD, Kiss M, Hershey J, et al. Chest tube insertion: a prospective evaluation of pain management. Clin J Pain. 1998;14(2):152-154.
- Gerner P. Postthoracotomy pain management problems. Anesthesiol Clin. 2008;26(2):355-367, vii.
- Blanco R, Parras T, McDonnell JG, et al. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia. 2013;68(11):1107-1113.
- Maximum Recommended Doses and Duration of Local Anesthetics. Accessed October 22, 2020. https://medicine.uiowa.edu/iowaprotocols/maximum-recommended-doses-and-duration-local-anesthetics
- Liu X, Song T, Xu H-Y, et al. The serratus anterior plane block for analgesia after thoracic surgery: A meta-analysis of randomized controlled trails. Medicine. 2020;99(21):e20286.
- Durant E, Dixon B, Luftig J, et al. Ultrasound-guided serratus plane block for ED rib fracture pain control. Am J Emerg Med. 2017;35(1):197.e3-e197.e6.
Oliver Hulland, MD
Yale New Haven Hospital
Jessica Oswald, MD, MPH
Center for Pain Medicine
Department of Emergency Medicine
Department of Anesthesia
University of California San Diego Health


