From Buzzwords to Operations: The Practical Use of Grounded AI Tools for EUS Leaders
Joshua Kaine, MD
Indiana University School of Medicine
Artificial intelligence (AI) has become a hot topic in the public eye and within healthcare. Two recent articles in the ACEP Emergency Ultrasound (EUS) newsletter helped us understand the “AI alphabet soup” and the current state of billing and reimbursement related to AI.1,2 Building on that foundation, this article focuses on how we, as POCUS leaders, can use grounded AI tools in a practical way to support the operational work of an EUS program.
Understanding AI
Broadly speaking, AI refers to computer systems capable of performing tasks that typically require human intelligence—such as pattern recognition, language processing, and decision support.3 In practice, AI shows up in several forms, including computer vision (image analysis) and large language models (LLMs) such as ChatGPT, Gemini, and Claude.
These models are trained on large volumes of data to generate statistically likely responses. Importantly, they do not understand content in a human sense and so they can sometimes “hallucinate,” producing answers that sound plausible but are incorrect or fabricated. For emergency ultrasound leaders, the goal is not an AI that sounds smart. The goal is an assistant that is auditable, conservative, and rooted in verifiable sources.4
GPTs and grounding – it’s all about the constraint
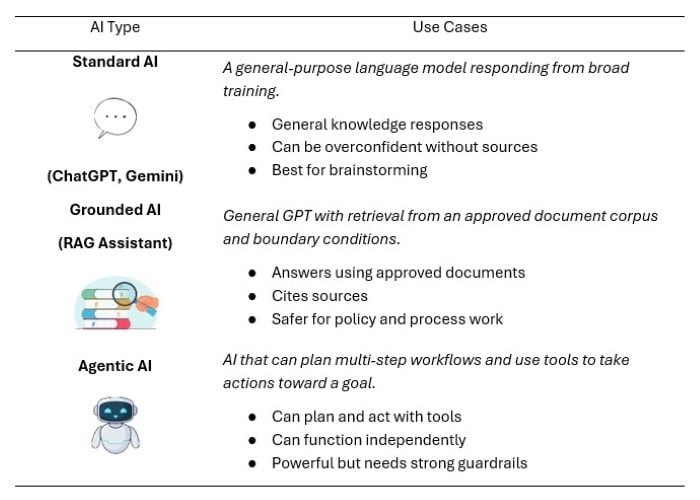
General-purpose AI tools (ChatGPT, Gemini, etc.), trained on broad data, can be excellent for brainstorming, drafting, and high-level overviews. However, they may not reliably cite sources and can be vulnerable to hallucinations when asked detailed policy, process, or documentation questions.
This is where grounding becomes useful. Grounding constrains the system to answer using a defined corpus of reference documents (often called retrieval-augmented generation, or RAG). When done well, this approach can reduce hallucinations and makes responses more verifiable because the model is summarizing from specific sources rather than improvising.
You may also hear the term AI agent used in this space and it’s worth asking “why not just build an agent?” In general, an AI agent is designed to do more than answer questions: it can chain multiple steps, use tools, and sometimes plan and take actions toward a goal (eg, generating a report, updating a log, or running an automated workflow). An agent is empowered to act and to do. A grounded assistant (RAG), by contrast, primarily retrieves and summarizes from an approved document set so its output is easier to audit and verify. For EUS operations, that tradeoff matters. We usually want constrained answers with traceable sourcing, not autonomous behavior. Agent-style automation may be valuable in future iterations (e.g. drafting monthly QA summaries or compiling policy updates), but it also increases complexity and risk if the system can act beyond the reference corpus. In high-stakes operational domains like disinfection and documentation, constraint is the feature.
For EUS program leaders, that grounded document set can be curated to include policies, processes, and guidelines that matter day-to-day: ACEP and AIUM guidance, CDC disinfection recommendations, manufacturer instructions for use (IFUs), and local institutional policies. Thus, a grounded assistant behaves differently from a general chatbot in that it answers only when it can point back to a source within the approved corpus. When it cannot, it should say so plainly.
Verified truth – how a grounded assistant can impact a POCUS program
How many times as a POCUS leader have you been asked which wipe can be used to clean a certain probe? You then must locate the device’s IFU and decode which products are compatible. A grounded assistant can help retrieve and summarize the relevant sections quickly while still pointing back to the IFU as the source of truth.
Similarly, when billing/coding leaders ask what documentation elements are needed to support a given exam, or new faculty ask about minimum documentation requirements, a grounded assistant can provide consistent templates and checklists aligned with your reference documents. Providing answers to high-frequency operational questions is where grounded tools can shine. Each answer should be traceable to a policy, guideline, or operating manual, improving standardization and reducing policy drift.
Demo: a guideline-grounded EUS policy & compliance assistant
To explore this idea, I built a guideline-grounded assistant (using Gemini “Gems”) designed specifically for emergency ultrasound operations. It is focused on documentation, disinfection/reprocessing, and best-practice questions. The assistant is grounded in ACEP policy, AIUM position statements, CDC guidance, a CPT reference set, and operating manuals/IFUs from major manufacturers (eg, SonoSite, Mindray, Philips, Butterfly, GE). It uses a source hierarchy where manufacturer IFUs and local policies supersede broader national guidance when there is conflict, to provide the most practical and actionable responses.
Try the demo here: https://tinyurl.com/bddz7cmv (requires logging into a Google account)
Note: This is an educational/operational demo. Verify alignment with local policy and the applicable manufacturer IFU. If you pilot this locally, start by loading your institution’s infection control policy and the IFUs for the specific probes in your fleet.
What it’s designed to do
- Answer policy/operations questions using a defined set of reference documents
- Provide structured outputs (checklists, templates) where appropriate
- Encourage conservative behavior (ask clarifying questions; avoid assumptions)
What it’s not designed to do
- Provide patient-specific medical advice
- Interpret images or make diagnoses
- Recommend treatment or clinical management
- Replace local infection control or compliance expertise
Future iterations: the next step isn’t “smarter,” it’s “more constrained”
AI is evolving rapidly, with new tools appearing frequently. As clinicians and operational leaders, we should demand systems that are accurate, bounded, and auditable before incorporating them into clinical workflows or administrative structures. My hope is that this article offers one concrete approach to AI integration by starting with a guideline-grounded assistant aimed at operational questions. In operational leadership, constraint is the feature. The more clearly we define sources, scope, and guardrails, the more useful these AI tools become.
References
- Liu RB, Baloescu C. Making sense of the AI alphabet soup in POCUS. ACEP Emergency Ultrasound Section Newsletter. February 2026. https://www.acep.org/emultrasound/newsroom/february-2026/making-sense-of-the-ai-alphabet-soup-in-pocus
- Guttman J. AI in POCUS: An overview of the current billing and reimbursement. ACEP Emergency Ultrasound Section Newsletter. February 2026. https://www.acep.org/emultrasound/newsroom/february-2026/ai-in-pocus-an-overview-of-the-current-billing-and-reimbursement
- Maiter A, Alabed S, Allen G, Alahdab F. AI in healthcare: an introduction for clinicians. BMJ Evid Based Med. 2025;30(6):376-80. doi: 10.1136/bmjebm-2024-112966. PMID: 39863401.
- Patel MR, Balu S, Pencina MJ. Translating AI for the Clinician. JAMA. 2024;332(20):1701-2. doi: 10.1001/jama.2024.21772. PMID: 39405321