

Expecting Frostbite, Getting Tropical Parasites: The Realities of Being an Antarctic Expedition Doctor
Dalton Wren, FP-C, CCP-C
Department of Integrative Physiology, University of Colorado Boulder
Kelly Wren, MD, MS
Emergency Medicine and Expedition Physician
Three weeks into an Antarctic expedition, we learned that the universe has a very dark sense of humor. At 2230, the Assistant Expedition Leader knocked on our cabin door. She timidly asked if we were still awake and if we could talk in the infirmary. Once inside, she unwrapped a 24-cm Ascaris lumbricoides worm (Figure 1 below) that she had just spontaneously defecated. It turns out that you don’t need to be in a tropical jungle to find a tropical parasite, you just need a patient who recently returned from one.
Ascaris, a parasitic roundworm, is the world’s most successful hitchhiker. While it usually plays nice, it has the potential to cause volvulus, intussusception, appendicitis, cholecystitis, pancreatitis, cholangitis, hepatic abscess and surgical emergencies that we are not equipped to manage on our ship. In endemic areas, these worms are reported to be responsible for nearly half of all biliary disease.1
But there we were, surrounded by icebergs, staring at a nematode that was very much outside of its latitude. Fortunately, she was pain free. On our POCUS scan her gallbladder was dilated but consistent with her fasting state and her wall measurements were within normal limits. Most importantly, there was no evidence of a writhing “tube in a tube” structure in her biliary tree.
In the other six continents, the easy solution is a 400-mg tablet of albendazole and a follow-up appointment. However, we were the Drake’s Passage away from the nearest pharmacy and unsurprisingly, we discovered that no Ushuaia pharmacies stocked it. We spent the next few days coordinating a way to get the medication flown from Buenos Aires to Ushuaia ensuring it would meet the ship upon our scheduled arrival. But as any wilderness medic knows, pathology rarely waits for logistics. Before we could reach the "Fin del Mundo" she developed acute abdominal pain. She remained stable without any localizing findings on physical examination or POCUS. She subsequently disembarked in Ushuaia and was flown to Buenos Aires for definitive care. She was treated without complication, but we kept her sidelined for two weeks post-treatment and required a repeat medical exam and clearance before she could return to the vessel. A worm-induced bowel obstruction is not something you want to troubleshoot in
20-foot swells. This case served as a stark reminder that our medical kits need to be as cosmopolitan as our crew members are. While we pack for frostbite and falls, adding albendazole to the kit is prudent as most wilderness guides are by nature true world explorers.
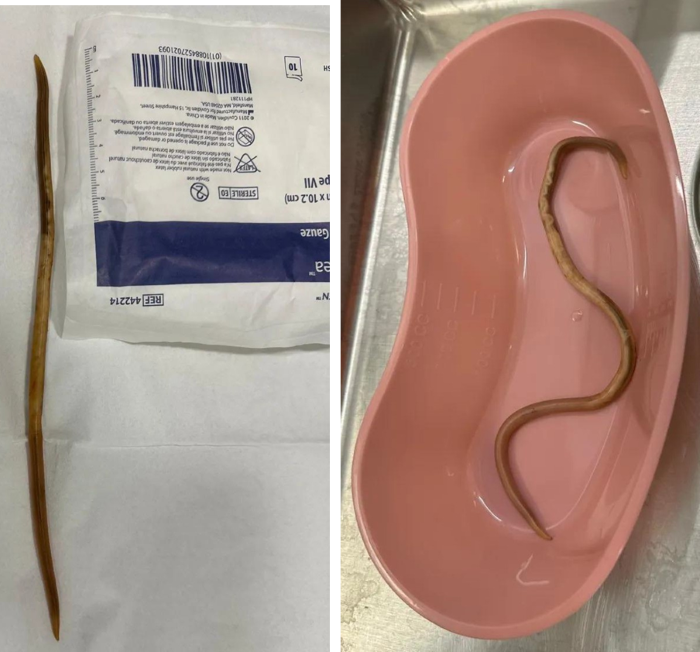 Figure 1. 24-cm Ascaris lumbricoides worm
Figure 1. 24-cm Ascaris lumbricoides worm
1 Jourdan PM, Lamberton PHL, Fenwick A, Addiss DG. Soil-transmitted helminth infections. Lancet. 2018;391(10117):252-265. https://doi.org/10.1016/S0140-6736(17)31930-X


