

Medical Response in Two Active Shooter Scenarios
After Action Report Analysis of the Aurora Century 16 Theater Shooting and the Marjory Stoneman Douglas High School Shooting
Mikayla Myers, MD Candidate 2023, Joan C Edwards School of Medicine
Reena Park, MD Candidate 2023, Joan C Edwards School of Medicine
Statistics have shown a continuous rise in the number of mass shooting incidents in the United States over the last decade (Valeeva., et al, 2022). In these active shooter scenarios, law enforcement (LE) is tasked with initial situational analysis, scene security, and requesting further resources (i.e. emergency medical services) to respond (IACP, 2018). With the uncertainty of imminent threats in these active shooter incidents, law enforcement officers (LEOs) are often the first to enter the scene and, in turn, the first to come in contact with injured victims. Unlike LEOs, traditional emergency medical service (EMS) providers are not trained or equipped to handle high threat situations. The rescue task force (RTF) and tactical emergency medical support (TEMS) concepts were developed to address the delay in medical care for victims of violent attacks. Early medical intervention and rapid transportation to an appropriate treatment facility are the most important factors to limit the loss of life (IACP, 2018). Although there is much variability among incidents, identifying patterns will aid in understanding the most effective ways to provide rapid medical care to victims of these incidents.
In this paper, we examine two active shooter incidents, the Aurora Century 16 Theater shooting, and the Marjory Stoneman Douglas High School shooting to:
- Evaluate which first responders (LE, EMS, specialized RTF, or TEMS) provided the first medical care.
- Identify which agency provided the majority of early medical care.
- Identify which agency provided care to the majority of critical patients.
- Analyze the efficacy of traditional EMS, RTF, and TEMS responses in these specific situations.
Early medical care is an important parameter as the most critical injuries must be treated rapidly to minimize death. It is important to know which agencies provided care to the most critical patients as these are the injuries that are time sensitive. With the advent of innovative EMS systems to address the high threat environment, we must analyze their efficacy in real-life situations.
On July 20, 2012, a mass shooting led to the death of 12 victims and injury to 82 others inside a Century 16 movie theater in Aurora, Colorado, United States.
On February 14, 2018, a devastating school shooting resulted in the death of 17 victims and the injury of 17 others at the Marjory Stoneman Douglas High School in Parkland, Florida, United States.
Both of these events demonstrated law enforcement’s prompt medical intervention, while the response from traditional and innovative medical care systems including EMS, TEMS, and RTF was delayed. The following gives us a closer look at the provision of medical care in these active shooter events.
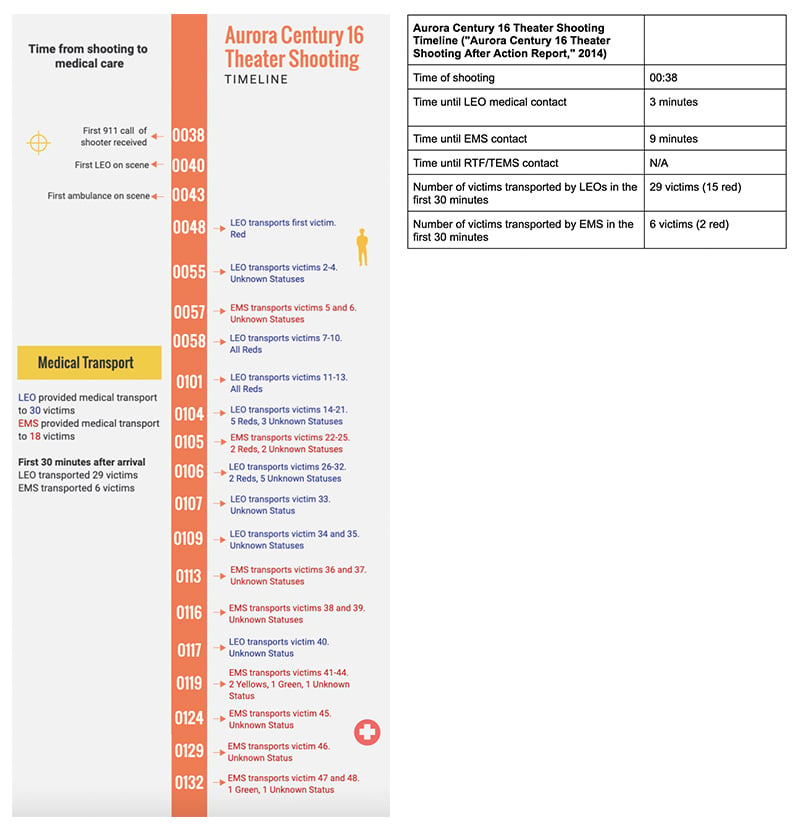
In the Aurora Century 16 Theater shooting, the Aurora Police Department (APD) was the first to arrive at the scene, enter the theater and make contact with, at a minimum the first seven reported victims. LEOs in Aurora did not have medical training or supplies, with the exception of a police officer, who was also trained as a S.W.A.T paramedic and was incidentally in the initial wave of LEOs to reach the location of the shooting. The officer had initially responded as a member of the APD, but at some point, transitioned from his law enforcement role to his medical role inside the theater.
Ten minutes after the initial 911 call of the shooting and eight minutes after law enforcement’s arrival, the first victim was transported to the hospital via police vehicle. Although this is not standard procedure for many police departments, LEOs quickly recognized the serious condition of the victim and the need for higher level medical care. Despite EMS arrival at the scene within three minutes of being dispatched, medical care and adequate transportation were delayed. Ambulances were unable to reach designated areas as a result of parked police vehicles and civilians fleeing the scene. In addition, uncertainty about the safety of the area meant EMS was unable to enter the theater.
Therefore, the first victim's transport by ambulance did not take place until a full fourteen minutes after EMS arrival. In this time, law enforcement officers had already transported three additional victims by police vehicle. Between the eighteen- and twenty-four-minutes following law enforcement’s arrival at the scene, police transported twelve additional critical victims despite six ambulances being staged on scene that did not transport during this time frame.
It was unclear from the After Action Report, which of the limitations in this situation primarily motivated the final mutual decision to continue transport via police vehicle to the hospital but, ultimately, police would end up carrying out both the initial triage and transport of thirty of the sixty victims (fifteen of which were critically injured) directly to the hospital despite no training beyond basic first aid and no medical supplies in their vehicles ("Aurora Century 16 Theater Shooting After Action Report," 2014). Law enforcement transported the majority of victims to the hospital and also the majority (almost 90%) of all critical patients. Eighteen of the sixty victims were transported by ambulance (two of which were critically injured) and the other twelve arrived at the hospital by private vehicle or had unknown modes of transportation.
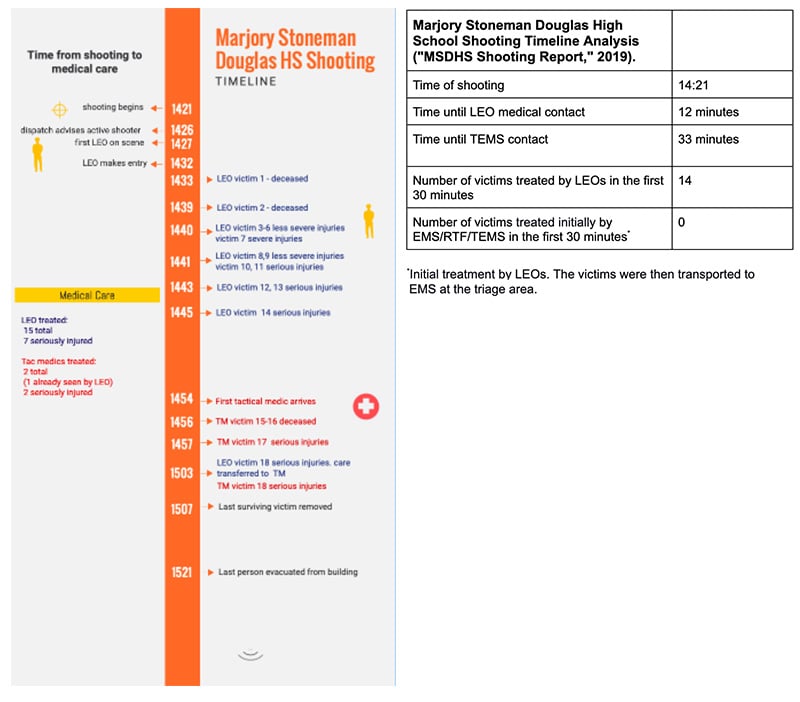
In the Marjory Stoneman Douglas High School shooting, Coral Springs Police Department law enforcement officers were the first to make medical contact with victims, twelve minutes after the onset of the shooting and one minute after arriving on the scene. The officers on scene supplied early emergency medical care and rapidly extricated victims. Law enforcement established initial medical contact with fourteen victims within the first thirty minutes and treated a total of fifteen of the seventeen victims.
Because of scene insecurity, EMS was staged outside. EMS made the critical decision to not delay definitive care with extensive medical treatment when victims were brought to them at the triage site. Rather, they coordinated and provided the crucial rapid transportation of all victims brought to them in the triage area by LEOs.
Throughout the MSD shooting, Building 12, where the shooting occurred, was designated as a hot zone, therefore the incident commander decided not to deploy RTF teams into the school.
Tactical medics made medical contact with victims thirty-three minutes after the shooting started and over twenty minutes after the first law enforcement entry into the school. Tactical medics treated two victims, one of which had already been seen by LEOs.
Analysis
Law Enforcement Medical Response
In both active shooter events, law enforcement officers provided the most rapid care AND care to the majority of critical or seriously injured victims.
Sometimes LEO care meant tourniquet and chest seal application. Other times, it simply meant recognition of injury severity and rapid transportation to a hospital, which also proved to be life-saving. While traditional EMS is typically not equipped or trained to enter a high threat scene, LEOs, since the Columbine High School shooting, are trained to rapidly enter an active shooter scene and decisively neutralize the threat. This critical action prevents further casualties. However once accomplished, as demonstrated in the Marjory Stoneman Douglas High School and Aurora Century 16 Theater shootings, this places LEOs immediately in contact with victims needing medical help in the hot zone without the assistance of EMS. Whether LEOs feel medical care is part of their job or not, these cases show they were nonetheless faced with this responsibility. Undoubtedly, lives were saved by law enforcement’s quick action in both of these cases.
EMS Medical Response
In both situations, traditional and innovative EMS access to patients was delayed.
Traditional EMS is not trained or equipped to enter an unsafe scene; therefore, other models have been considered to expedite access to critical patients during a high threat event. Two widely recognized innovative EMS models are rescue task force (RTF) and tactical EMS (TEMS).
Typically, the RTF is composed of LEOs and Fire/EMS; law enforcement’s defined role in the RTF is to provide protection while fire/EMS treats victims in the warm zone. RTF is not approved to enter hot zones. Experience has taught us that determining if a scene is “warm” in a chaotic situation is often difficult. This limitation was evident in the case of the Marjory Stoneman Douglas High School shooting where RTF was assembled and asked to respond in the school yet was denied entry because the scene was deemed "hot."
The tactical medical provider’s mission is to preserve the well-being of tactical operators. TEMS providers are often associated with S.W.A.T. There are many variations on the theme of first responders dual trained in law enforcement and medicine. A TEMS provider may be a law enforcement officer cross trained as a paramedic, a physician who is also a sworn law enforcement officer, or a paramedic with extra tactical-EMT training. The TEMS provider may move into hot zones with S.W.A.T., or they may be best situated in an armored vehicle at the scene. Their medical capabilities can range from the level of a paramedic to that of the highest-level physician.
S.W.A.T. teams, however, require time to assemble. In active shooter response, the first officers on scene are often expected to make rapid entry and not wait on S.W.A.T. teams to form. The first arriving officer on scene is often proximity dependent and likely to be a patrol officer. Similarly, the first responding EMS agency will likely be the agency in closest proximity to the event and unlikely to be a TEMS provider.
As was seen in the case of the Aurora Century 16 Theater shooting, a TEMS medic-trained law enforcement officer incidentally made early entry. This entry was not part of a coordinated S.W.A.T team response but rather a fortunate coincidence. At the Marjory Stoneman Douglas High School shooting, S.W.A.T along with the tactical medics arrived on scene much later than the non-S.W.A.T. officers and did not make medical contact with any victims until thirty-three minutes after the start of the shooting and after the majority of victims had already been treated by LEOs.
Conclusion
The "Golden Hour" and "Platinum Half-Hour" are windows of time that emphasize the urgency required for a trauma victim to receive definitive medical care before morbidity and mortality significantly increase (Nickson, 2020). Both the Aurora and MSD shootings demonstrated that law enforcement officers were the first to arrive on the scene in these high threat situations and the first to make medical contact with victims. For a variety of reasons already discussed, traditional EMS and even innovative RTF and TEMS medics encountered difficulties accessing patients quickly in these situations.
These two incidents demonstrate the importance of training and equipping law enforcement in basic tactical emergency casualty care medical skills and mass casualty care to respond to high threat events. They also demonstrate the importance of unified command and interagency training.
Moving forward, to reduce preventable deaths, more incidents should be reviewed specific to medical response in high threat events. All first responder roles should be reassessed with the end-goal of closing the gap in medical care during high threat events. More research focusing on detailed medical aspects of these incidents should be conducted. Lastly, frank, and creative, evidence-based interagency discussions on all levels from federal to local must be had to discuss future responses to high threat events.
References
- https://www.themarshallproject.org/2022/07/06/what-you-need-to-know-about-the-rise-in-u-s-mass-shootings
- https://www.theiacp.org/sites/default/files/2018-08/ActiveShooterPaper2018.pdf
- https://www.courts.state.co.us/Media/Opinion_Docs/14CV31595%20After%20Action%20Review%20Report%20Redacted.pdf
- https://www.fdle.state.fl.us/MSDHS/CommissionReport.pdf
- https://litfl.com/trauma-mortality-and-the-golden-hour/


