

Hip to It!: The Role of POCUS in Evaluating Pediatric Hip Pathology
Alyssa Goodman, MD, MPH
Joni E. Rabiner, MD
Munaza Batool Rizvi, MD, FAAP, RDCS, Editor
Case presentation
A 6-year-old previously healthy male presents to the pediatric emergency department (PED) with acute onset of a right-sided limp and fever. He had a recent viral upper respiratory infection but has had no known trauma. On physical examination, he is in mild pain and febrile to 39.3C. His physical examination is significant for right hip pain with flexion and external rotation. Point-of-care ultrasound (POCUS) of the right hip is performed to assess for hip effusion. (Figure 1)
 Figure 1. Point-of-Care Ultrasound (POCUS) demonstrating hip effusion
Figure 1. Point-of-Care Ultrasound (POCUS) demonstrating hip effusion
Background
Point-of-care hip ultrasound is an objective and quantitative method for assessment of hip pathology in children. This rapid, non-invasive modality allows bedside detection of hip effusions. Some of the diseases that can commonly cause hip effusions include transient synovitis, septic arthritis, Lyme disease, osteomyelitis, and osteonecrosis. Given the ease of performing this quick study at the bedside, it has become a tool that pediatric emergency medicine (PEM) physicians use in the acute setting.1 The hip can be assessed on POCUS to evaluate for effusion, and bony abnormalities may be seen as well.
Technical Approach
To perform a hip ultrasound, children should be supine with the leg slightly externally rotated. (Figure 2A) The linear or curvilinear transducer may be used, depending on the size of the child and the depth of the femur. The transducer is placed on the anterior hip, in the sagittal position, parallel to the long axis of the femoral neck, just distal to the inguinal crease, with the probe marker oriented cranially and pointing towards the umbilicus.2 The femoral head is seen as a curvilinear, hyperechoic line with posterior acoustic shadowing and may have a physis. The femoral neck is seen as a hyperechoic, linear bone with posterior acoustic shadowing just distal to the femoral head. If there is any difficulty locating the femur in the longitudinal view, the transverse view may be used to locate the femur as a hyperechoic, curvilinear line with posterior acoustic shadowing, and then the probe can be turned 90 degrees to image the femoral head and neck in the longitudinal view. For comparison, the contralateral normal hip can be evaluated as well for effusion.
Pain control and distraction techniques may help to obtain images and to minimize the patient’s discomfort. Distraction techniques include use of warm gel, having the patient lay in a parent/guardian lap, music or visual aids for distraction, and child life involvement. Clinicians should monitor for discomfort during positioning or acquisition as not to worsen any injury or discomfort.
Pediatric Hip Anatomy
In B-mode, the landmarks for hip ultrasound that should be identified include the hyperechoic curvilinear femoral head (with or without a physis), the femoral neck, and the iliopsoas muscle. (Figure 2B) The bone appears hyperechoic with posterior acoustic shadowing. The physis of the femoral head appears as a regular, V-shaped indentation in the femoral head. The anterior synovial recess overlies the femoral neck. There is a femoral fat pad as well as joint capsule between the iliopsoas muscle and the femoral neck, and this is a potential space for fluid or effusion to accumulate.3 In a normal hip, there may be some fluid over the femoral head, but there will not be any fluid over the femoral neck.
 Figure 2A. Linear probe position for performing POCUS of the hip to evaluate for hip effusion
Figure 2A. Linear probe position for performing POCUS of the hip to evaluate for hip effusion
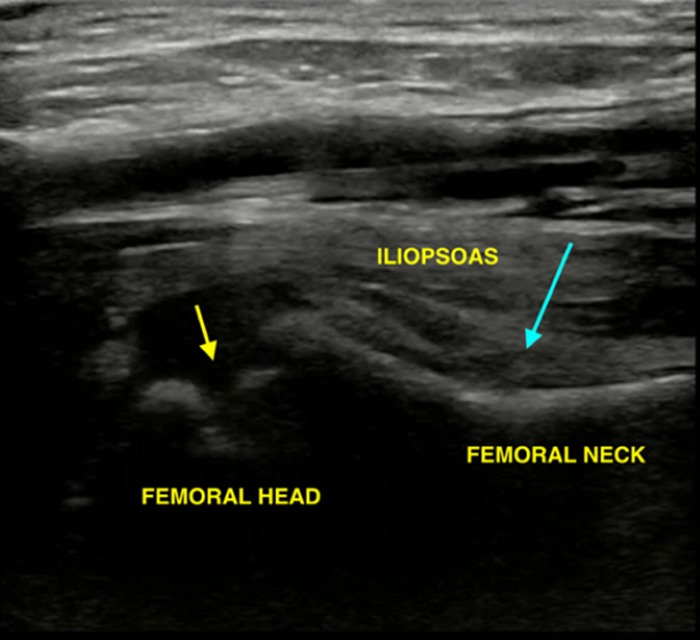 Figure 2B. Normal hip anatomy (small yellow arrow: physis of the femoral head, long blue arrow: anterior synovial space).
Figure 2B. Normal hip anatomy (small yellow arrow: physis of the femoral head, long blue arrow: anterior synovial space).
Hip Effusion
A hip effusion can be identified as anechoic fluid in the anterior synovial space between the femoral neck and the posterior surface of the iliopsoas muscle. The criteria for diagnosis of a hip effusion are fluid measuring > 5 mm or > 2 mm of fluid difference between the affected and the contralateral normal hip. There is some debate regarding measurement technique. Effusions may be measured either directly across the hypoechoic fluid or from the anterior surface of the femoral neck to the posterior surface of the iliopsoas muscle. (Figure 3) However, clinically significant effusions will likely be positive (> 5 mm) regardless of measurement technique, and asymmetry of the bilateral hips will usually be visually evident. In addition, hip effusions generally have a convex shape, with fluid accumulating in the joint capsule, compared to the normal joint capsule without fluid that appears concave. It is often helpful to evaluate the bilateral hips simultaneously with the dual screen technique, which allows for a direct, side-by-side comparison of the bilateral hips. (Figure 4) Color Doppler may be applied to the effusion to confirm the presence of fluid and to rule out vascular pathology.
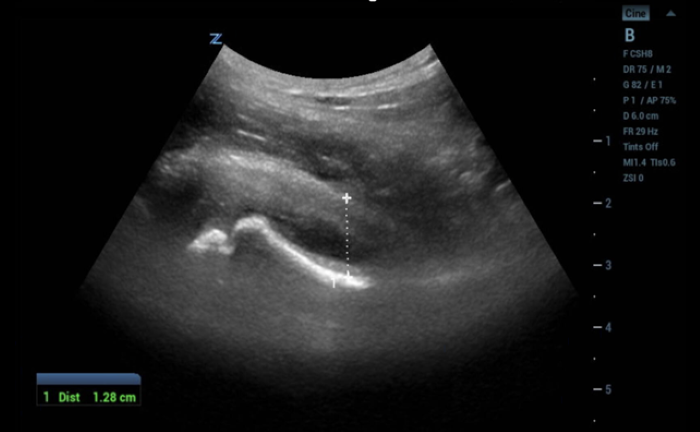 Figure 3A. Hip effusion measuring 12.8 mm, measured from the anterior surface of the femoral neck to the posterior surface of the iliopsoas muscle.
Figure 3A. Hip effusion measuring 12.8 mm, measured from the anterior surface of the femoral neck to the posterior surface of the iliopsoas muscle.
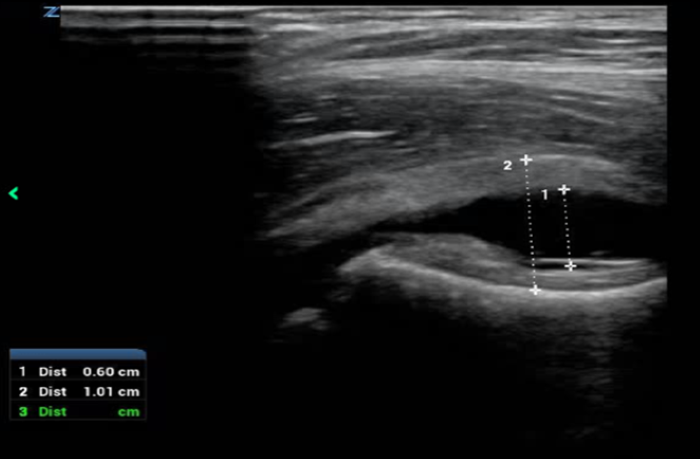 Figure 3B. Comparison of hip effusion measurements with measuring the hypoechoic fluid directly (measurement 1 = 6 mm) vs. measuring from the anterior surface of the femoral neck to the posterior surface of the iliopsoas muscle (measurement 2 = 10 mm).
Figure 3B. Comparison of hip effusion measurements with measuring the hypoechoic fluid directly (measurement 1 = 6 mm) vs. measuring from the anterior surface of the femoral neck to the posterior surface of the iliopsoas muscle (measurement 2 = 10 mm).
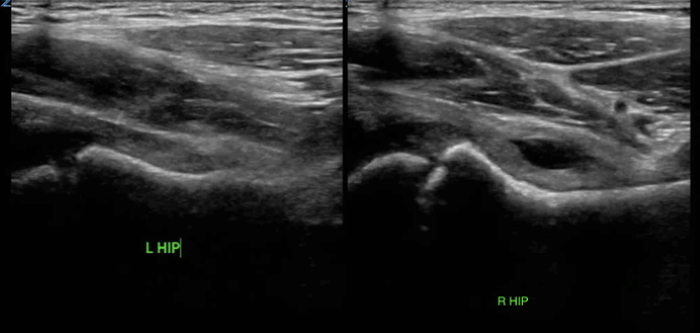 Figure 4. Dual screen technique for direct comparison of bilateral hips.
Figure 4. Dual screen technique for direct comparison of bilateral hips.
Limitations of Pediatric Hip Ultrasound
There are several limitations of pediatric hip ultrasound. The etiology of the effusion cannot be determined, and the complete clinical picture must be considered. Hip effusions may be due to trauma, infectious, or inflammatory etiologies. In addition, infectious and inflammatory etiologies can vary from orthopedic emergencies such as septic arthritis to benign conditions such as transient synovitis. Further workup, including laboratory studies, further imaging, and/or orthopedics consultation, may be indicated for definitive diagnosis.
Clinical and Research Applications
Research has highlighted the utility of hip POCUS across both pediatric and adult patients.
Hip POCUS has been shown to have high diagnostic accuracy when assessing for a hip effusion in the PED. A recent multicenter prospective study of 161 children with hip pain compared POCUS with radiology-performed ultrasound and demonstrated a sensitivity of 94% and specificity of 98%. In this study, hip POCUS was performed by 18 PEM physicians, with 3 high-volume physicians enrolling 62% of patients. When comparing the high-volume physicians to the remaining 15 physicians, the sensitivity ranged from 98% for the high-volume enrollers to 83% for the remaining physicians, while specificity was 98% for the high-volume physicians and 97% for the remaining physicians. This suggests that while novice sonologists can perform hip US with good accuracy, there is a learning curve for hip POCUS.1
A retrospective pediatric study demonstrated that a novel POCUS decision-supported algorithm (POCUS-DSA) accurately identified transient synovitis of the hip. This study included 621 patients, 6 patients with septic arthritis, 4 with osteomyelitis, and 4 with Legg-Calve-Perthes disease. The sensitivity of POCUS-DSA for the diagnosis of transient synovitis was 91%, with a positive predictive value of 99%, and the specificity was 79%. POCUS was helpful for determining of the presence of an effusion and may save time on unnecessary bloodwork and further diagnostic imaging studies in the PED.4
Hip POCUS is increasingly being utilized in the adult ED for assessment of septic arthritis or other etiologies of hip pain. A study of adult patients presenting to the emergency department found that hip POCUS compared to radiology-performed US significantly decreased time to ultrasound and arthrocentesis, with time to ultrasound decreased from 209 minutes for radiology-performed ultrasound to 68 minutes for hip POCUS, and time to arthrocentesis decreased from 602 minutes for a radiology-performed arthrocentesis to 211 minutes in the POCUS/emergency physician-performed arthrocentesis group.5
Integration with Clinical Assessment
POCUS of the hip is a valuable tool in the pediatric emergency department. While hip POCUS can identify the presence of a hip effusion, the underlying etiology cannot be determined solely from POCUS imaging, and POCUS findings must be interpreted in the context of the patient’s overall clinical presentation. Validated decision-making frameworks such as the Kocher criteria (fever, inability to bear weight, ESR elevation, leukocytosis) may assist in distinguishing septic arthritis from transient synovitis. Hip POCUS can also be useful in the evaluation of undifferentiated leg pain in a child with a limp or non-specific leg pain by narrowing down the area of pathology. Therefore, this rapid bedside assessment for hip effusion can assist in establishing diagnosis and play a critical role in guiding appropriate management.
Case Resolution
His POCUS of the right hip was significant for an effusion measuring 7 mm (Figure 5), with no effusion appreciated on the left side. The differential diagnosis for this child with hip pain, fever, and hip effusion includes septic arthritis, transient synovitis, and trauma. Given the inability to bear weight, fever, and hip effusion on POCUS, laboratory tests were obtained that were significant for a leukocytosis of 15,000 cells/mm3 and an ESR of 52. As the Kocher criteria confirmed a high likelihood for septic arthritis and the hip POCUS showed an effusion, the patient had a hip arthrocentesis performed by orthopedics and intravenous antibiotics were started. Cultures obtained from the hip joint effusion confirmed a Methicillin-susceptible Staphylococcus aureus bacterial infection as the cause of his septic hip and antibiotics were tailored accordingly.
 Figure 5. POCUS image demonstrating a hypoechoic hip effusion overlying the femoral neck measuring 7 mm.
Figure 5. POCUS image demonstrating a hypoechoic hip effusion overlying the femoral neck measuring 7 mm.
Conclusions
In conclusion, hip POCUS is a non-invasive modality which provides an objective tool to assess for and measure hip effusions. Growing evidence supports its clinical utility across emergency department settings, both for pediatric and adult populations. Future research may further define its role in guiding diagnosis and help to establish protocols to integrate this application further into clinical practice.
Summary
- Hip POCUS measurements are taken on the affected side and the contralateral normal side for comparison.
- For hip ultrasound measurements, measure either the hypoechoic fluid directly or from the anterior surface of the femoral neck to the posterior surface of the iliopsoas muscle. Fluid measuring >5 mm or >2 mm difference compared with the contralateral hip suggests effusion.
- Use pain control and distraction techniques to limit discomfort from the POCUS examination.
References
- Jones RM, Malia L, Snelling PJ, et al. Diagnostic accuracy of point-of-care ultrasound for hip effusion: a multicenter diagnostic study. Ann Emerg Med. 2025;86(6):566-75. doi:10.1016/j.annemergmed.2025.04.033
- Lin-Martore M. PEM POCUS Series: Hip Effusion. Academic Like in Emergency Medicine blog. May 17, 2021. Accessed March 16, 2026. https://www.aliem.com/pem-pocus-series-hip-effusion/
- Crow A, Cheung A, Lam A, Ho E. Sonography for the investigation of a child with a limp. Australas J Ultrasound Med. 2010;13(3):23-30. doi:10.1002/j.2205-0140.2010.tb00160.x
- Zoabi M, Kvatinsky N, Shavit I. Evaluation of a point-of-care ultrasonography decision-support algorithm for the diagnosis of transient synovitis in the pediatric emergency department. JAMA Netw Open. 2021;4(7):e2116915. doi:10.1001/jamanetworkopen.2021.16915
- Thom C, Ahmed A, Kongkatong M, Moak J. Point-of-care hip ultrasound leads to expedited results in emergency department patients with suspected septic arthritis. J Am Coll Emerg Physicians Open. 2020;1(4):512-20. doi:10.1002/emp2.12167
- Alamdaran SA, Taheri-Nezhad M, Nouri A, et al. Role of ultrasound and inflammatory factors in the management of pediatric hip joint effusion. Pediatr Rheumatol Online J. 2023;21(1):146. doi:10.1186/s12969-023-00922-8
- Vieira RL, Levy JA. Bedside ultrasonography to identify hip effusions in pediatric patients. Ann Emerg Med. 2010;55(3):284-9. doi:10.1016/j.annemergmed.2009.06.527
- Cruz CI, Vieira RL, Mannix RC, Monuteaux MC, Levy JA. Point-of-care hip ultrasound in a pediatric emergency department. Am J Emerg Med. 2018;36(7):1174-7. doi:10.1016/j.ajem.2017.11.059
- Shavit I, Eidelman M, Tsafrir M, Eilam A, Segal D. Sonography of the hip joint by the emergency physician. Pediatr Emerg Care. 2006;22(8):570-3.


