
Ultrasound-guided Cricothyrotomy and a Novel 3-D Printed Training Model
Thomas Lawyer, MD, Ultrasound Fellow at Osceola Regional Medical Center / University of Central Florida in Kissimmee, FL
Javier Rosario, MD, FACEP, Co-Chair of Emergency Ultrasound Section Simulation Subcommittee, Ultrasound Division Director at Osceola Regional Medical Center / University of Central Florida in Kissimmee, FL
Background
Cricothyrotomy is a high acuity, low occurrence procedure that is reserved for scenarios in which the provider cannot intubate or oxygenate the patient. This procedure is classically performed by identifying the cricothyroid membrane (CTM) by palpation. Many patient factors including obesity make localization of the CTM by palpation difficult.1 Ultrasound has been shown to improve localization of the CTM, and both increase success rate and decrease complications of cricothyrotomy several fold.2,3 Procedural training for ultrasound-guided cric has been described using cadavers, animal, and combination plastic/meat models.4,5,6 Here we review the advantages of US guided cric and describe a novel 3-D printed ultrasound-guided cric training model.
Cricothyrotomy by Ultrasound Guidance vs Palpation Alone
EM physicians are familiar with the technique of performing cricothyrotomy after identifying the CTM by palpation. In 2012, Keith Curtis and colleagues described a novel technique of ultrasound-guided, bougie assisted cricothyrotomy in cadavers.7 In this study, operators viewed the laryngeal cartilaginous structures including the CTM with the linear ultrasound transducer in long axis, the CTM was cut with a scalpel under active ultrasound guidance, then the bougie and endotracheal tube (ETT) were passed. This study reported a success rate of 20/21 attempts and an average time to completion of 26.2 seconds. Others have described ultrasound guidance for percutaneous tracheostomy with the probe in a transverse orientation on the neck.8 Ultrasound has been shown to improve localization of the CTM, increase success rate and decrease complications of cricothyrotomy.2,3,9
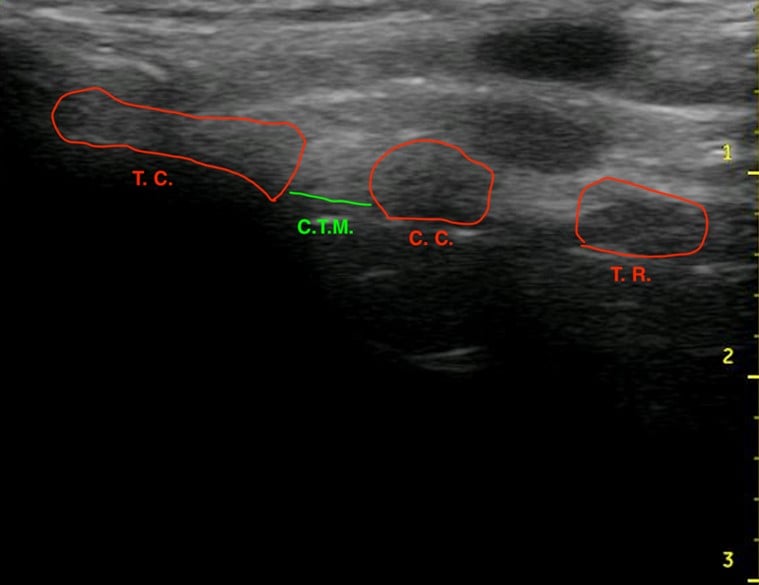
Figure 1.Ultrasound of the midsagittal plane of the anterior neck showing the thyroid cartilage (T.C.), cricothyroid membrane (C.T.M.), cricoid cartilage (C.C.), and the first tracheal ring (T.R.).
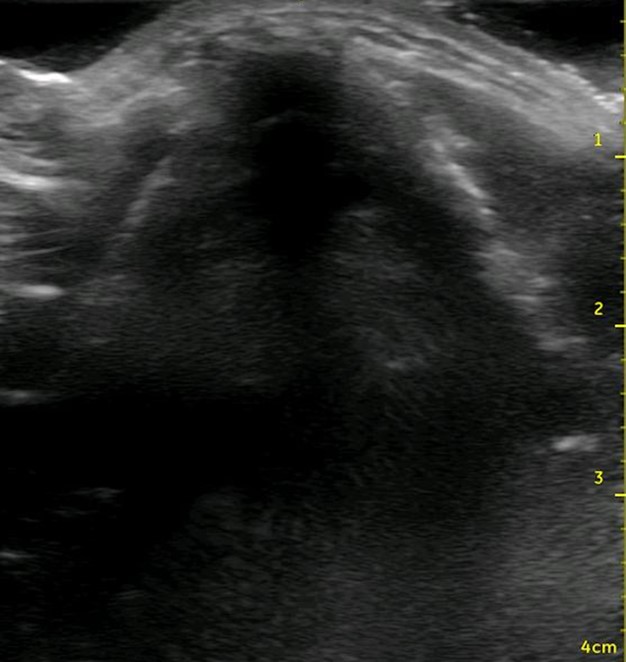
Figure 2. Ultrasound view of the thyroid cartilage in the transverse plane.
A Novel 3-D Printed Model for Ultrasound-guided Cricothyrotomy Training
Procedural training for ultrasound-guided cric has been described on cadavers, animal-derived and combination plastic/meat models, each model with its own advantages and drawbacks for use as a training model.4,5,6 Cadavers are realistic, but expensive, difficult to transport, and not re-usable. Animal derived and meat models also provide realistic anatomy but can be difficult to obtain and to store.

Figure 3. A porcine model for teaching ultrasound-guided cricothyrotomy
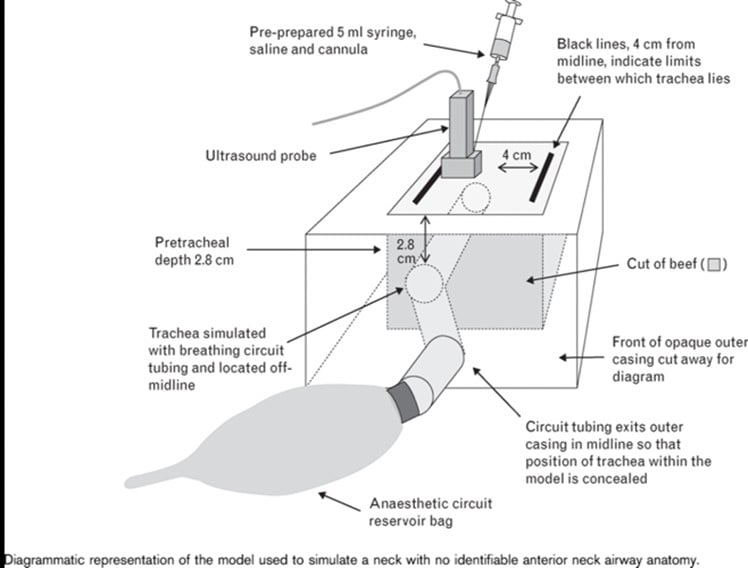
Figure 4. A combination plastic and meat-based model for teaching ultrasound-guided cricothyrotomy
Here we describe a novel model for US-guided cric training that uses 3-D printed structures to provide the realism of cadavers, and the re-usability and durability of synthetic models.
3-D printable designs for cricothyrotomy using the palpation method have been available for free for educational purposes online. Using a free download computer design program, a 3-D model of the neck was redesigned to allow for greater pre-tracheal soft tissue, to create a model where palpation of the landmarks for performing cric is difficult or impossible. This model was converted into a format to be printed on a 3-D printer. The 3-D printable components of this model can be found for free download for educational use on Thingiverse.com by searching for ultrasound guided cric trainer.
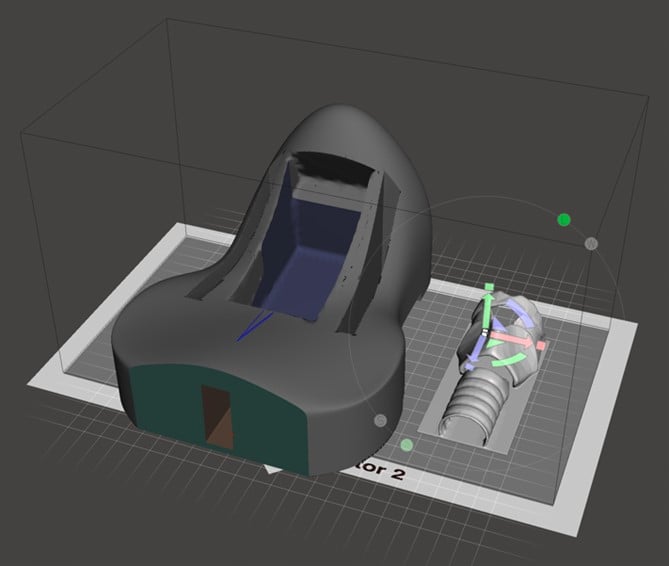
Figure 5. Computer model of neck and larynx as components of a task trainer for ultrasound-guided cricothyrotomy
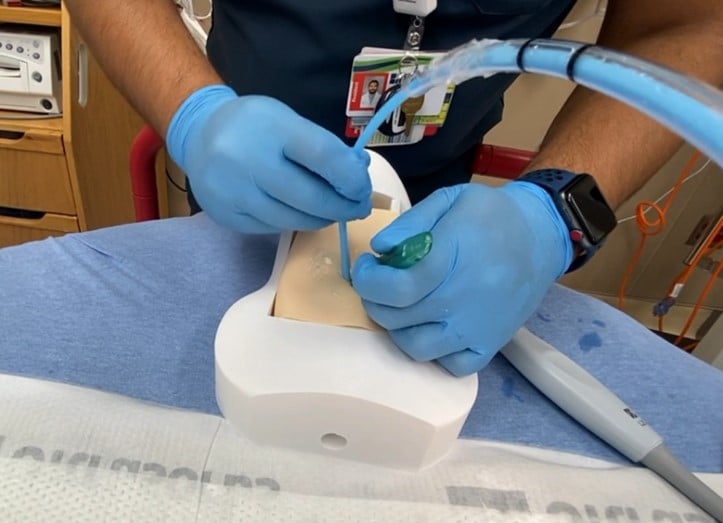
The model can be re-created by downloading the model for 3-D printing, and following the following steps:
- Print the neck model and riser blocks (used to vary the depth of pre-tracheal soft tissue, if desired) on the 3-D printer out of hard plastic polylactic acid (PLA) or similar material.

- Print the larynx on a 3-D printer out of more flexible thermoplastic polyurethane (TPU) or similar material. This allows for a more realistic feel of passing the tube through the larynx, without rigid plastic to for the tube to get caught on.

- Ballistic gel is available commercially with various firmness. Gel that mimics fat tissue works well for this application. Melt the gel in a pot to create slabs of gel of the desired thickness of pre-tracheal soft tissue. This model allows up to approximately 2.5 cm of pre-tracheal soft tissue. Once cool, cut the gel into slabs that fit the model.
- Create an artificial cricothyroid membrane on the model by covering the space for the CTM with a layer of tape.
- For a simulated difficult cricothyrotomy, consider placing the model larynx directly into the neck model without riser blocks behind it. This allows for the largest amount of space in front of the larynx to be filled with ballistic gel acting as pre-tracheal soft tissue.

- Apply generous amounts of ultrasound gel on top of the model larynx, and on top of the ballistic gel to optimize ultrasound images.

- Cut a piece of commercially available artificial skin to size to cover the ballistic gel and complete the model.

In contrast to native cartilage, which is hypoechoic with posterior shadowing, the plastic model of the thyroid cartilage and cricoid cartilage appear hyperechoic with more dense posterior shadowing (below). This model performs well as an ultrasound-guided cric training model. It has realistic anatomy. It models a patient with difficult to palpate anatomy, which are patient who may be difficult to intubate and may be more likely to need cricothyrotomy in the first place. The overlying skin and pre-tracheal ballistic gel can be easily and quickly replaced for the next operator in a training setting. The model allows for performing all the steps of cricothyrotomy including passing the bougie and ETT. The model is durable and re-usable.
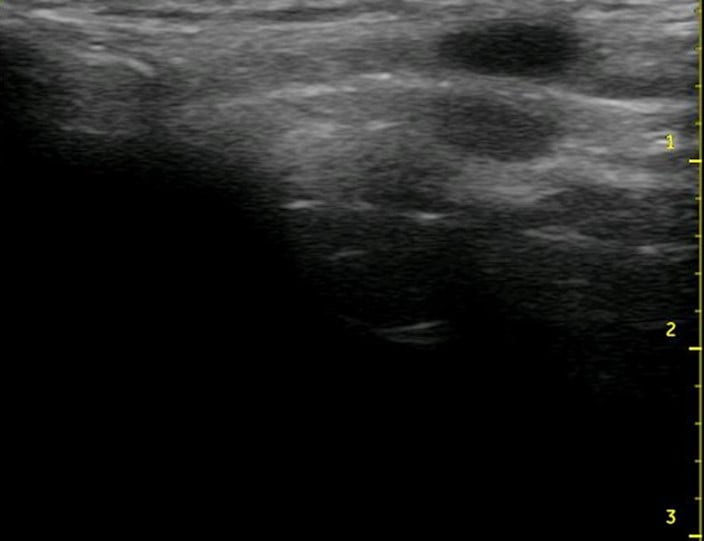
Figure 6. Midsagittal ultrasound of the anterior neck of a live person
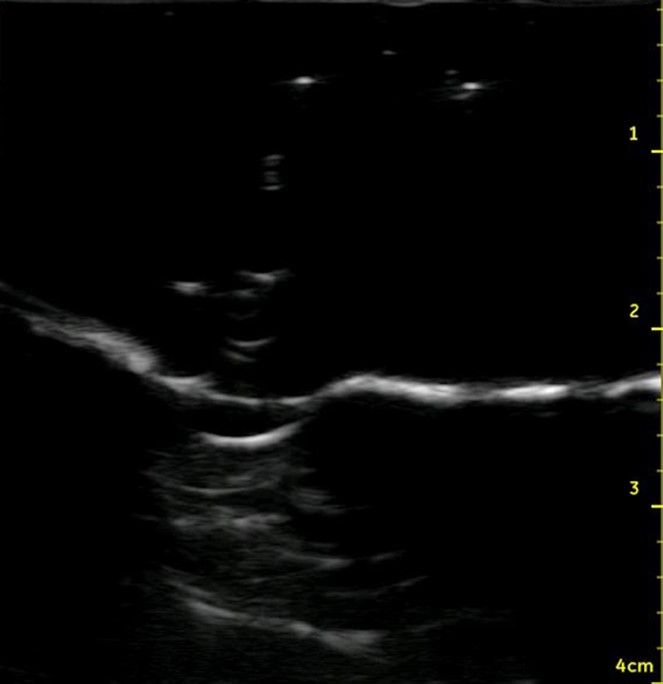
Figure 7. Midsagittal ultrasound of the anterior neck of the model
References
- You-Ten KE, Desai D, Postonogova T, Siddiqui N. Accuracy of conventional digital palpation and ultrasound of the cricothyroid membrane in obese women in labour. Anaesthesia. 2015;70:1230-4.
- Siddiqui N, Yu E, Boulis S, You-Ten KE. Ultrasound is superior to palpation in identifying the cricothyroid membrane in subjects with poorly defined neck landmarks: a randomized clinical trial. Anesthesiology. 2018;129(6):1132-9.
- Siddiqui N, Arzola C, Friedman Z, Guerina L, You-Ten KE. Ultrasound improves cricothyrotomy success in cadavers with poorly defined neck anatomy: a randomized control trial. Anesthesiology. 2015;123(5):1033–41.
- Takayesu JK, Peak D, Stearns D. Cadaver-based training is superior to simulation training for cricothyrotomy and tube thoracostomy. Intern Emerg Med. 2017;12(1):99-102.
- Mandell D, Orebaugh SL. A Porcine Model for Learning Ultrasound Anatomy of the Larynx and Ultrasound-Guided Cricothyrotomy. Simul Healthc. 2019;14(5):343-7.
- Dinsmore J, Heard AM, Green RJ. The use of ultrasound to guide time-critical cannula tracheotomy when anterior neck airway anatomy is unidentifiable. Eur J Anaesthesiol. 2011;28(7):506-10.
- Curtis K, et al. Ultrasound-guided, Bougie-assisted cricothyroidotomy: A description of a novel technique in cadaveric models. Acad Emerg Med. 2012;19(7):876-9.
- Rudas M, Seppelt I, Herkes R, Hislop R, Rajbhandari D, Weisbrodt L. Traditional landmark versus ultrasound guided tracheal puncture during percutaneous dilatational tracheostomy in adult intensive care patients: a randomised controlled trial. Crit Care. 2014;18(5):514.
- Elliott D, Baker P, Scott, M, Birch CW, Thompson J M. Accuracy of surface landmark identification for cannula cricothyroidotomy. Anaesthesia. 2010;65:889-94.


