Beyond Breath Sounds: How Diaphragmatic Ultrasound Predicts Pediatric Respiratory Outcomes
Elaine Chiang, MD
Boston Children’s Hospital
Joni E. Rabiner, MD
Columbia University, Vagelos College of Physicians and Surgeons
Article Editor: Munaza Batool Rizvi, MD, Columbia University, Vagelos College of Physicians and Surgeons
Case Presentation
A 7-month-old previously healthy male presents to the pediatric emergency department with cough, nasal congestion, and increased work of breathing for 2 days. On physical examination, he is tachypneic with mild intercostal retractions and has an oxygen saturation of 94% on room air. He has coarse breath sounds and wheezing diffusely. Point-of-care diaphragmatic ultrasound is performed to assess respiratory status. His ultrasound shows a reduced diaphragmatic thickening fraction (TF) of 28% and an increased inspiratory slope (IS) of 0.8 cm/s, both correlating with increased work of breathing and moderate-severe bronchiolitis.
Background
Point-of-care diaphragmatic ultrasound provides objective, quantitative assessment of diaphragmatic function and respiratory status in children. This non-invasive modality offers rapid, real-time information on diaphragmatic function. It has also been shown to correlate with disease severity in pediatric respiratory illnesses including bronchiolitis, pneumonia, and asthma and is gaining increased attention in both adult and pediatric emergency medicine and critical care units.
Technical Approach
The diaphragm is assessed using two complementary approaches from different views: diaphragmatic excursion (DE) in the subcostal view and diaphragmatic thickening (DT) in the midaxillary view. Children should be supine and breathing quietly, without crying, coughing, or speaking. Calming and distraction techniques are essential for obtaining quiet respiration. Measurements are obtained over 3 respiratory cycles and averaged. A slower M-mode sweep speed may capture all 3 cycles on one screen. Right-sided measurements alone are typically sufficient, as values are similar bilaterally and the left diaphragm is often obscured by the stomach.
Diaphragmatic Excursion (DE)
Diaphragmatic excursion (DE) measures the vertical displacement of the diaphragm during respiration. DE can be evaluated in the subcostal view. In this approach, a phased array or curvilinear probe is placed just below the right costal margin in the midclavicular line, with the probe marker oriented cranially. [Figure 1A] This brings the liver into view, which serves as an acoustic window for visualization of the dome of the diaphragm. The diaphragm will appear as a bright, hyperechoic curvilinear line superior to the liver.
In B-mode, the diaphragm contracts and moves downward toward the probe during inspiration, then relaxes and moves upward during expiration. In M-mode, with the cursor placed perpendicular to diaphragmatic motion, the diaphragm appears as a hyperechoic line with upward and downward deflections over time. [Figure 1B] The upward deflection ("peak") represents end inspiration; the downward deflection (“valley”) represents end expiration. Diaphragmatic excursion is measured as the vertical distance between these two points, averaged over 3 respiratory cycles. [Table 1] Normal reference values for DE in healthy children have been established and vary by age.
|
Parameter |
Formula |
|
Diaphragmatic Excursion (DE) |
Vertical displacement (cm): End inspiration position - End expiration position |
|
Diaphragmatic Thickening (DT) |
Thickness (cm): End inspiration - End expiration |
|
Thickening Fraction (TF) |
(Thickness end inspiration - Thickness end expiration) / Thickness at end expiration × 100 |
|
Inspiratory Slope (IS) |
(Inspiratory excursion in cm) / (Inspiratory time in seconds) |
|
Expiratory Slope (ES) |
(Expiratory excursion in cm) / (Expiratory time in seconds) |
Table 1. Diaphragmatic Ultrasound Parameters and Formulas
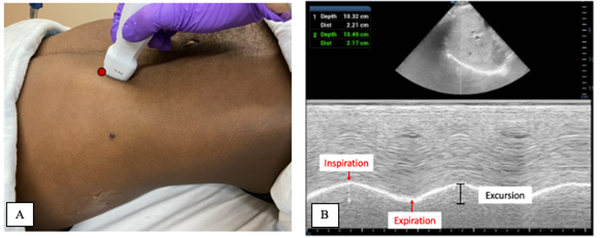
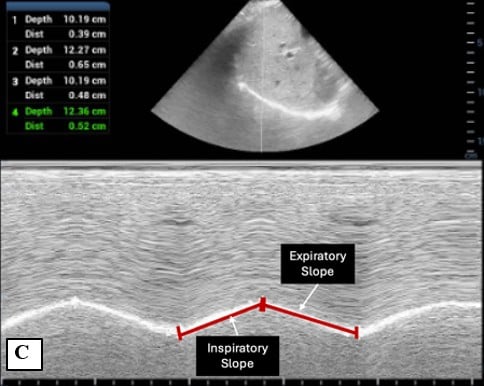
Figure 1. Probe placement and M-mode evaluation of diaphragmatic excursion 2
A) Probe placement in subcostal view for evaluation of diaphragmatic excursion.
B) Diaphragmatic excursnspiratory and expiratory slope
C) Inspiratory and expiratory slope
Inspiratory Slope (IS) and Expiratory Slope (ES)
Inspiratory and expiratory slopes quantify the velocity of diaphragmatic contraction and relaxation, respectively. Evaluated in sub-costal view, they are calculated using the total duration of the respiratory cycle on M-mode. [Table 1] [Figure 1C] While IS and ES have been studied in pediatric respiratory illnesses and show correlation with disease severity, normal reference values for healthy children have not yet been established.3-5
Diaphragmatic Thickening (DT)
Diaphragmatic thickening can be evaluated in the midaxillary view in the zone of apposition, where the diaphragm attaches to the rib cage. In this approach, a high frequency linear probe is placed in the 9th to 10th intercostal space in the right midaxillary line with the probe marker oriented cranially. [Figure 2A] The diaphragm appears as a hypoechoic muscular layer bordered by two hyperechoic lines representing membranes of the pleura and peritoneum. [Figure 2B]
During inspiration, these hyperechoic lines move apart as the diaphragm thickens; during expiration, they move closer together as it thins. In M-mode, measure the distance between the pleural and peritoneal membranes (from the inner aspect of one echogenic line to the inner aspect of the other)6 at end inspiration and end expiration over 3 respiratory cycles, then average the values. [Table 1] [Figure 2B] Age-based normal reference values for DT and thickening fraction (TF) have been established.1
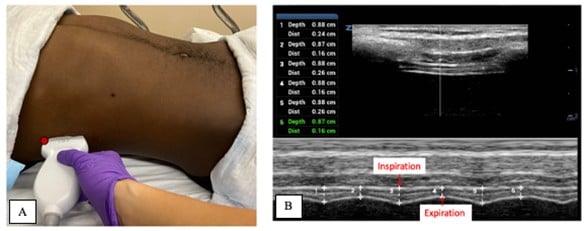 Figure 2. Probe placement and M-mode evaluation of diaphragmatic thickening82
Figure 2. Probe placement and M-mode evaluation of diaphragmatic thickening82
Training and Quality Considerations
Expert consensus recommends 40 supervised examinations before performing diaphragmatic ultrasound independently for clinical or research purposes.6 This threshold reflects the technical skill required for consistent, reproducible measurements.
Key quality considerations includes
- Patient cooperation: Quiet breathing required; crying or coughing limits accuracy
- Body habitus and positioning: Obesity may reduce image quality; keep patient supine throughout measurement
- Ventilator effects: PEEP reduces excursion and increases resting thickness
- Measurement location: Measure at the same intercostal space for serial assessments
- Timing: Measure at thickest and thinnest diaphragm states
- M-mode cursor: Place perpendicular to diaphragmatic motion
- Thickness measurement: Between (not including) pleural and peritoneal membranes
- Context-specific interpretation: Normal thickening fraction ranges depend on whether the patient is breathing spontaneously or receiving ventilatory support
Clinical and Research Applications
Emerging research has highlighted the broad utility of diaphragmatic ultrasound across adult and pediatric emergency and intensive care settings. While evidence is accumulating, most applications remain under investigation.
In adult emergency departments, diaphragmatic ultrasound assesses respiratory muscle function, predicts respiratory failure, and guides ventilator management. For example, one study of patients with COPD exacerbations found that those with thickening fraction <20% were more likely to require positive pressure ventilation, with a high sensitivity (84.6%) and specificity (91.5%).7
In the pediatric emergency department, diaphragmatic ultrasound has been shown to correlate with disease severity in bronchiolitis, pneumonia, and asthma. A study of diaphragmatic ultrasound in children with bronchiolitis showed that TF, IS and thickness at end inspiration correlated with need for supplemental oxygen and respiratory support.3 Another study of children with bronchiolitis showed that DE, IS, and ES correlated with clinical and sonographic severity scores, and IS was also found to predict hospital length of stay.4 For pneumonia in children, one study showed that IS, ES, and TF correlated with clinical scores and hospital length of stay.5 Lastly, for asthma in children, another study showed that DT and TF correlated with disease severity.2
In the intensive care setting, diaphragmatic ultrasound has been used to assess diaphragmatic dysfunction in mechanically ventilated patients. Studies have shown that TF and DE can detect atrophy and predict extubation success.8-10 The American Academy of Pediatrics endorses diaphragmatic ultrasound for evaluating diaphragm motion and function in neonates with respiratory compromise.11
Integration with Clinical Assessment
Diaphragmatic ultrasound provides valuable objective data to enhance standard clinical assessment. To optimize clinical utility:
- Recognize common artifacts: Cardiac motion may appear in subcostal views; awareness allows appropriate interpretation
- Enhance clinical correlation: Integrate findings with established clinical severity scores for comprehensive assessment
- Leverage serial measurements: Track trends over time to guide patient management and monitor response to therapy
Case Resolution
Based on the reduced TF of 28% and elevated IS of 0.8 cm/s, both associated with greater disease severity, the patient was started on high-flow nasal cannula and admitted for respiratory support. These findings predicted need for escalated care and longer hospital stay, consistent with published literature.3,4
After 24 hours, the patient showed clinical improvement with decreased work of breathing and improved oxygen saturation. Repeat diaphragmatic ultrasound demonstrated objective improvement: TF increased to 42% and IS decreased to 0.4 cm/s. These quantitative changes paralleled clinical recovery and supported the decision to wean respiratory support.
Conclusion
In conclusion, diaphragmatic ultrasound is a non-invasive modality which provides an objective tool for assessing diaphragm function and respiratory illness severity. Growing evidence supports its clinical utility across critical care and emergency department settings in both the adult and pediatric populations. Future research may further define its role in guiding respiratory management and establish baselines and protocols to integrate this application into clinical practice.
Key Clinical Points
- Diaphragmatic ultrasound measurements need to be taken during quiet breathing, with no crying, coughing, or speaking
- Diaphragmatic excursion (DE): M-mode cursor is placed perpendicular to the direction of motion of the diaphragm and the difference between end inspiration and end expiration is measured
- Diaphragmatic thickening (DT): M-mode cursor is placed over the diaphragm in the zone of apposition, where the diaphragm attaches to the chest wall
- Measurements are taken over 3 respiratory cycles and averaged
- Consider 40 supervised exams for competency development
- Use as an adjunct to established clinical assessment tools
- Serial measurements may provide more valuable trending data than isolated values
References
- El-Halaby H, Abdel-Hady H, Alsawah G, Abdelrahman A, El-Tahan H. Sonographic Evaluation of Diaphragmatic Excursion and Thickness in Healthy Infants and Children. J Ultrasound Med. 2016;35(1):167-75.
- Chiang E, Kessler DO, Liebman M, Rabiner JE. Diaphragmatic Ultrasound in Children With Asthma Exacerbations. Pediatr Emerg Care. 2024;40(8):603-6.
- Buonsenso D, Supino MC, Giglioni E, et al. Point of care diaphragm ultrasound in infants with bronchiolitis: A prospective study. Pediatr Pulmonol. 2018;53(6):778-86.
- Şık N, Çitlenbik H, Öztürk A, et al. Point of care diaphragm ultrasound in acute bronchiolitis: A measurable tool to predict the clinical, sonographic severity of the disease, and outcomes. Pediatr Pulmonol. 2021;56(5):1053-9.
- Şık N, Çitlenbik H, Öztürk A, et al. Point of care diaphragm ultrasound: An objective tool to predict the severity of pneumonia and outcomes in children. Pediatr Pulmonol. 2021;56(6):1666-72.
- Haaksma ME, Smit JM, Boussuges A, et al. Expert consensus on diaphragm ultrasonography in the critically ill (EXODUS): a Delphi consensus statement on the measurement of diaphragm ultrasound-derived parameters in a critical care setting. Crit Care. 2022;26(1):99.
- Kocyigit H, Gunalp M, Genc S, et al. Diaphragm dysfunction detected with ultrasound to predict noninvasive mechanical ventilation failure: A prospective cohort study. Am J Emerg Med. 2021;45:202-7.
- Valverde Montoro D, García Soler P, Hernández Yuste A, Camacho Alonso JM. Ultrasound assessment of ventilator-induced diaphragmatic dysfunction in mechanically ventilated pediatric patients. Paediatr Respir Rev. 2021;40:58-64.
- Lee EP, Hsia SH, Hsiao HF, et al. Evaluation of diaphragmatic function in mechanically ventilated children: An ultrasound study. PLoS One. 2017;12(8):e0183560.
- Arslan G, Besci T, Duman M. Point of care diaphragm ultrasound in mechanically ventilated children: A predictive tool to detect extubation failure. Pediatr Pulmonol. 2022;57(6):1432-9.
- Stewart DL, Elsayed Y, Fraga MV, et al. Use of Point-of-Care Ultrasonography in the NICU for Diagnostic and Procedural Purposes. Pediatrics. 2022;150 (6):e2022060053.