

Disaster Medicine Section Newsletter: Summer 2026 Edition
Table of Contents
- Letter from the editors
- Call for student/trainee and early career author submissions
- Disaster medicine lecture series
- From the Field: Jamaica Hurricane Response
- Frontline Spotlight: Dr. Ariel Kaim
- Disaster committee update
- Mentorship program
Letter from the Editors
Disasters do not recognize borders. Pandemics, geopolitical conflict, climate-driven events, and cyberattacks impact people across nation state borders and best prevention, mitigation and response practices come from international cooperation and shared learning.
This edition highlights the global nature of disaster medicine and the importance of looking beyond our borders and learning from our international colleagues who navigate in diverse systems and have alternate views, experiences and expertise. From a hurricane response in Jamaica to an Israeli expert discussing disaster research to an upcoming lecture from a South Korean physician who started a disaster medicine institute in his country, these experts offer a unique perspective.
By sharing knowledge across borders, we strengthen preparedness, improve response, and build more resilient healthcare and emergency response systems together. And as humans we grow from building these meaningful friendships and relationships.
In addition to the written format, we are expanding into podcasting some content (thanks to Dr. Hata!) to provide physicians with content that can be accessed during commutes, workouts, travel, or between shifts. Check out Dr. Arielle Kaim’s podcast on real time evaluation of disaster medicine response and disaster medicine research https://on.soundcloud.com/kfIbUoGHnzjYMaTDSO and read more about her work in the newsletter.
Our next newsletter is broadly themed to showcase early career physician authors. Please consider contributing or mentoring an upcoming disaster medicine leader by submitting to the newsletter. More details below.
Lastly, we want to broadcast your experience and expertise. Do you have a deployment or response to share? Perhaps some preparation for an event or a particular kind of disaster? We look forward to hearing from the good work you are doing.
Humbly,
Ryan Hata, MD
Dominique Wong, MD
Call for Student/Mentor Newsletter Submissions

Our next newsletter edition will highlight student, trainee and early career voices in disaster medicine. We are seeking brief articles, reflections, case insights, and creative perspectives. If you’re a student, resident, fellow or early career physician—or mentor collaborating with one—share your work and help showcase the next generation of leaders in the field.
We welcome submissions including:
- Original articles on disaster preparedness, response, or recovery
- Reflections on training experiences, field exercises, or mentorship
- Case studies highlighting initiatives or academic projects
- Creative perspectives — essays, infographics, or visual storytelling related to disaster medicine education
Please submit your articles to Amber Hartman @ ahartman@acep.org by August 15, 2026.

Disaster Medicine Lecture Series
Disasters evolve fast—and so should your readiness.
Our Disaster Medicine Lecture Series delivers insights from experienced frontline clinicians, responders, and operational leaders. Hone your readiness, gain new medical knowledge, increase your awareness, or simply hear fascinating first-hand perspectives from experts across disaster medicine.
Upcoming dates and topics:
July 21 12-2 pm CT
- Dr. Heejun Shin: From Fellow to Director: Translating Disaster Medicine Fellowship into Practice, Education, and Leadership
- Dr. Al Hakmani Haitham: Hospital Preparedness and Health System Resilience: Practical Leadership Lessons from Disaster Medicine
August 18 12-2pm CT
- Dr Sandy Schneider: Improving Diffusion of Clinical Care Innovations in Public Health Emergencies
- Dr. Kyle Herbert : The Role of the National Guard in Disaster Response
See more upcoming lecture topics and speakers and register here: https://www.acep.org/administration/ems-resources/disaster-medicine-lecture-series
From the Field: Disaster Medicine Reflection: Lessons From the Israeli Medical Team Response to Hurricane Melissa in Jamaica, 2025
Lea Ohana Sarna Cahan
Department of Pediatric Emergency Medicine, Hadassah Hebrew University
Medical Center, Jerusalem, Israel.
Hebrew University Medical Center, Faculty of Medicine, Hebrew University of
Jerusalem, Israel
Giselle Watt
Accident & Emergency Department, Mandeville Regional Hospital, Mandeville, Jamaica
Joseph Mendelovic
Ministry of health Israel
Shaare Zedek Medical Center, Affiliated with the Hadassah-Hebrew University
School of Medicine, Jerusalem, Israel
Background
Hurricane Melissa caused widespread damage across Jamaica, on 28 October 2025,causing severe damage across western Jamaica and affecting nearly 1.6 million people, with 45 confirmed deaths reported and infrastructure damage estimated cost of USD 64.3 million. One of the most significant impacts was the functional destruction of Black River Hospital, which became nonoperational following flooding and structural damage. This abrupt loss of capacity resulted in a rapid surge ofpatients at Mandeville Regional Hospital and Saint Ann’s Bay Regional Hospital,both of which became primary referral centers during the response.1

Deployment team included a 30-member Israeli medical delegation, led by the Israeli Ministry of Health, to support the national response on the island during a two-week deployment. From a personal perspective, clinical work in a severely resource-constrained hospital setting following a large-scale disaster revealed a striking resemblance to the core principles of pediatric emergency medicine practiced in high-pressure environments worldwide. In conditions of sustained overload and limited diagnostic and therapeutic resources, physicians and multidisciplinary teams are compelled to move away from algorithmic or automated care and instead rely on advanced clinical judgment. As in the training and ethos of pediatric emergency medicine, each investigation is carefully considered with respect to its true necessity and potential impact on management. Clinical decision-making is deeply integrated with social and contextual factors, particularly when weighing the risks and feasibility of discharge versus hospitalization. Paradoxically, it is precisely within this scarcity-driven reality that bedside point-of-care ultrasound (POCUS) becomes even more critical than in resource-rich settings. Its ability to provide rapid, actionable information at the bedside underscores the urgent need to further develop and expand POCUS capacity in such environments.

Injury Patterns and System Strain
Although the total number of casualties was relatively limited, the impact on the healthcare system was substantial. With Black River Hospital offline, surge capacity was absorbed almost entirely by the remaining hospitals, stretching staffing, physical space, and diagnostic resources far beyond baseline levels. Patient presentations followed the classic three-phase injury pattern observed after natural disasters. The immediate phase was characterized by traumatic injuries related to flooding, debris, and environmental exposure.
The subacute phase was marked by a surge in morbidity related to disruption of routine and life-sustaining medical care. Patients presented with wound infections, dehydration, respiratory illnesses, and exacerbations of chronic diseases. Several cases illustrated the severity of these indirect effects. A young patient with chronic kidney disease missed scheduled dialysis due to infrastructure damage and transportation barriers, collapsed shortly after arrival to ED, and suffered cardiac arrest. Prompt, coordinated resuscitation resulted in successful return of spontaneous circulation, followed by stabilization and transfer to the intensive care unit. Inparallel, patients with diabetes mellitus presented with diabetic ketoacidosis, reflecting interruption of medications access and routine monitoring. Pediatric patients also presented with acute asthma exacerbations, likely triggered by environmental exposure, stress, and limited access to medications and follow-up care. Together, these cases highlighted how the subacute phase of disasters is often dominated by preventable, life-threatening complications of chronic disease.
The late phase includes evolving public health consequences, including challenges in continuity of pediatric services, increasing psychological stress, and the emergence of waterborne and vector-associated illnesses. Flooding, standing water, and disrupted sanitation create conditions conducive to these diseases, further burdening already strained healthcare facilities.

Collaboration, Clinical Excellence, and Workforce Fatigue
A central lesson from this mission was the importance of integrating with local healthcare teams, rather than operating in parallel. Working closely with physicians and nurses at Mandeville Regional Hospital, it became clear that disaster response success depended not on technology alone, but on the presence of highly trained clinicians capable of adapting to low-resource environments. Despite limited diagnostics, supply constraints, and sustained surge conditions, local teams demonstrated strong clinical reasoning, prioritization skills, and professionalism - hallmarks of resilient emergency care systems.

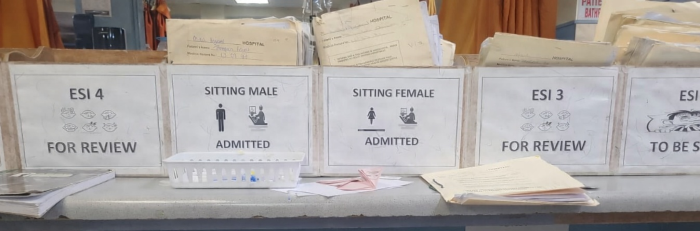
The deployment required rapid adjustment to an unfamiliar clinical environment with limited resources. Clinical decision-making relied more heavily on bedside assessment due to constrained diagnostics, and workflows shifted from electronic medical records to paper-based documentation. This adaptation highlighted the importance of flexibility and close collaboration when practicing disaster medicine in resource-limited settings.
To support bedside decision-making, we implemented just-in-time (JIT) point-of-care ultrasound (POCUS) training, tailored to trauma assessment, volume status evaluation, and cardiopulmonary complaints. In this low-resource context, POCUS served as a force multiplier, enhancing diagnostic confidence and supporting timely clinical decisions when advanced imaging was unavailable or delayed.
Operational continuity was challenged by significant healthcare worker fatigue and low morale throughout the response. Many staff members worked prolonged shifts with minimal rest while simultaneously coping with personal losses, including damage to their homes and family life. Importantly, mutual support within the healthcare system, through peer collaboration and visible solidarity between local and international teams, played a critical role in mitigating burnout.
The response to Hurricane Melissa highlighted the added value of close collaboration between local and international medical teams. Integrating into existing systems, rather than working in parallel, strengthened clinical decision-making, improved patient flow, and supported overstretched staff.
References:
1. Pan American Health Organization & World Health Organization. (2025, November 13). Hurricane Melissa in Jamaica: Situation Report No. 16.
Disaster Medicine Reflection: Lessons From the Israeli Medical Team Response to Hurricane Melissa in Jamaica, 2025
Frontline Spotlight

Arielle Kaim
Dr. Arielle Kaim is a lecturer, academic advisor, and researcher in the Department of Emergency Management and Disaster Medicine at the School of Public Health, Faculty of Medicine, Tel Aviv University. Her main research interests include emergency preparedness and response, disaster medicine, disaster management, and individual and community resilience. She is the author of over 40 full papers published in peer-reviewed, high-impact journals and has presented at leading national and international conferences. In addition, she serves as a senior consultant to the Israeli Ministry of Health and the European Commission. Dr. Kaim has also worked and deployed in field hospital deployments, refugee camps and underserved communities, most recently in Mozambique.
Listen to her podcast here or by scanning this QR code:

Dr. Kaim writes:
A central issue that warrants greater academic and operational attention is the persistent gap between the growing body of evidence in disaster medicine and its effective integration into practice. This challenge is especially relevant in the context of Emergency Medical Teams (EMTs), which are classified by the World Health Organization to provide rapid, quality-assured medical response in both international and domestic emergencies. Since the establishment of the WHO EMT Initiative in 2013, important progress has been made in strengthening standards, coordination mechanisms, classification processes, and the overall professionalization of the field. Nevertheless, substantial gaps remain in the systematic generation, translation, and integration of evidence into decision-making, training, and operational response.
A related challenge concerns how to make research more compelling, feasible, and operationally relevant within disaster medical deployments, particularly in settings where teams are working under extreme pressure and responding to immediate life-saving needs. Although the value of research is increasingly recognized, real-time data collection in the field is often perceived as an added burden rather than an integral component of response. This raises a critical question for the field: how can research be designed in ways that are methodologically rigorous, yet sufficiently practical, streamlined, and minimally disruptive to operational realities? In this sense, the issue is not only whether research can be conducted during deployments, but how it can be embedded in ways that demonstrate clear and immediate value to responders themselves.
My research engages directly with these challenges through a focus on the real-time evaluation of EMT disaster medical response. Specifically, I examine how actionable evidence can be generated during ongoing deployments to support adaptive learning, improve operational effectiveness, and strengthen the quality and accountability of response efforts. More broadly, this work seeks to contribute to a shift toward more systematic, impact-oriented, and evidence-informed approaches in disaster medicine, while also helping to position research not as an external academic exercise, but as a practical tool for improving response operations and, ultimately, patient care and outcomes.
Disaster Committee Update
Dr. Romeo Fairley, MD, MPH, FACEP
The ACEP Disaster Medicine Committee met on May 8, 2026, to review major strides in subspecialty development, operational resources, and crisis policies. To support the subspecialty development, the committee has drafted a mock core curriculum for an in-person review course and is currently partnering with the ACEP education team to build a supporting question bank. Additionally, efforts to promote the Disaster Medicine subspecialty are underway, and a robust new disaster medicine resource repository has been compiled and is awaiting an upcoming website redesign.
On the operational front, progress continues updating the Hospital Disaster Assessment Guide to make it more ED-specific and transition it into a fillable PDF, which will be submitted as an ACEP26 Pre-Conference proposal. The committee is also advancing active shooter protocols, with a new white paper heading to leadership for review following collaboration with the Tactical and Law Enforcement Section. Meanwhile, workgroups are actively revising the 2013 Guidelines for Crisis of Care and developing a standardized state policy template for allocating scarce medical resources during crisis situations. In policy updates, the committee has officially sunsetted the policy regarding the use of donated or self-purchased PPE during COVID-19.
Looking ahead to ACEP26 in Chicago, members can look forward to the EMS and Disaster Preconference on Sunday, October 4, from 8:00 AM to 5:00 PM at Chicago Fire.
Grow Your Career in Disaster Medicine
Interested in Disaster Medicine but unsure where to start? Looking for guidance on fellowship training, research, operational response, leadership opportunities, or career development?
The ACEP Disaster Medicine Section is developing a new mentorship program designed to connect members with experienced Disaster Medicine professionals from a variety of clinical, academic, operational, military, and public health backgrounds.
Whether you're a medical student, resident, fellow, early-career physician, or established professional seeking expertise in a new area, this program will provide valuable mentorship, networking opportunities, and career guidance.
The mentorship program will officially launch on August 3, 2026, with mentor and mentee enrollment opening at that time. We look forward to helping build the next generation of Disaster Medicine leaders and fostering meaningful connections across the Disaster Medicine community


