
Central Retinal Artery Occlusion
Drue M. Orwig, DO, MBA, CWSP
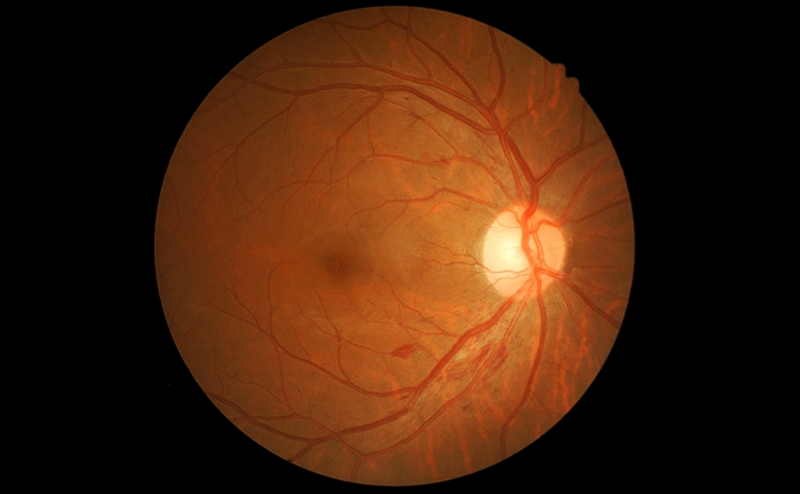
Central retinal artery occlusion (CRAO) is a rare and devastating diagnosis of severe monocular visual loss. Historically, there have been several treatments used to salvage visual function, such as ocular massage, hemodilution, and anterior chamber paracentesis. None of these, however, has been shown to improve outcomes compared to a control in experimental models.1 Clinically significant visual improvement with CRAO is considered to be ≥0.3 logMAR (about 1-3 steps on a standard US Snellen chart). Recently, researchers have looked at new treatments to improve visual acuity in these patients — intravenous alteplase and hyperbaric oxygen therapy (HBOT). Two articles from 2025 will be reviewed that evaluate both modalities as potential vision-saving interventions to consider in the future.
The first study published in the Lancet Neurology looked at the use of alteplase IV versus oral aspirin for acute CRAO.2 This was a 16-stroke site study in France enrolling patients with suspected non-arteritic acute CRAO. Patients were given either oral aspirin or alteplase IV if presented within 4.5 hours of symptom onset. Sixty-six percent of the alteplase group and 48% of the aspirin group showed improvement in visual acuity of at least 0.4 logMAR at 1 month follow up. Although not statistically significant, there was a noticeable trend toward improved outcomes in the alteplase IV group.

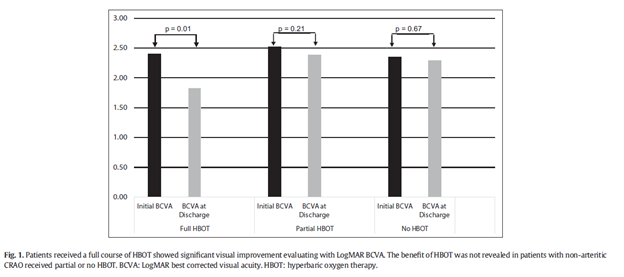
A second article published in the American Journal of Emergency Medicine by D. Orwig et al is one of several recent retrospective articles looking at HBOT for CRAOs.3 The FDA approved use of HBO for CRAO in 2006 (level IIB recommendation both per the American Heart Association and the Undersea and Hyperbaric Medical Society). HBO is able to supply 100% of the retinal oxygen needs through the choroidal circulation.4 This allows intermittent perfusion during a hyperbaric session to help keep the retina viable until the vessel recannulates. This retrospective review compared patients with full (twice daily HBOT for 5 consecutive days), partial, or no hyperbaric treatment course for CRAO. Patients had to present within 24 hours of onset. Patients that received a full course of HBOT experienced a significant visual improvement at discharge as observed on a logMAR best corrected visual acuity.
There have been several other recent retrospective reviews evaluating HBO for CRAO, most of which show improvement in visual acuity.
While the results of these studies are encouraging, more research utilizing both modalities is needed to see if either will truly change the prognosis of this disease.
- Cugati S, Varma DD, Chen CS, Lee AW. Treatment options for central retinal artery occlusion. Curr Treat Options Neurol. 2013 Feb;15(1):63–77.
- Préterre C, Gaultier A, Obadia M, et al; THEIA collaborators. Intravenous alteplase versus oral aspirin for acute central retinal artery occlusion within 4·5 h of severe vision loss (THEIA): a multicentre, double-dummy, patient-blinded and assessor-blinded, randomised, controlled, phase 3 trial. Lancet Neurol. 2025 Nov;24(11):909-919. doi: 1016/S1474-4422(25)00308-4. PMID: 41109232.
- Patz A. Oxygen inhalation in retinal arterial occlusion; a preliminary report. Am J Ophthalmol. 1955 Dec;40(6):789–795.
- Orwig DM, Wang J, Li Z, et al. The effects of hyperbaric oxygen treatment for non-arteritic central retinal artery occlusion (HBOT-CRAO). Am J Emerg Med. 2025 Dec;98:1-5. doi: 1016/j.ajem.2025.07.065. Epub 2025 Aug 5. PMID: 40784185.


