

June 2026 Sports Medicine Newsletter
Approach to the Pediatric Elbow in the Emergency Department
Charles Heinzmann, MD
University of Illinois College of Medicine Peoria
OSF Saint Francis Medical Center, Department of Emergency Medicine
Case Introduction
A 6-year-old male presents to the emergency department after falling from monkey bars at school. He complains of elbow pain and refuses to move his right arm. On exam, there is mild swelling around the elbow without obvious deformity. Neurovascular examination is intact. Radiographs are obtained, and the emergency physician begins a systematic evaluation of the pediatric elbow.
 Figure 1
Figure 1
 Figure 2
Figure 2
Case courtesy of Bálint Botz, Radiopaedia.org, rID: 61596
Pediatric elbow injuries are among the more challenging musculoskeletal complaints encountered in the emergency department. The complexity arises from multiple ossification centers, evolving skeletal anatomy, and subtle radiographic findings that can easily be mistaken for normal developmental changes. Missing an elbow injury may lead to long-term complications including malunion, growth disturbance, neurovascular compromise, or chronic functional impairment (1).
Initial radiographs should include an anteroposterior (AP) and lateral view of the elbow. Separate imaging of the humerus and forearm is often necessary to reveal the full extent of potential injuries (2). A structured and consistent approach to pediatric elbow radiographs can help rapidly identify common injuries and avoid diagnostic pitfalls. One practical framework includes evaluating four major components in sequence:
- Are the fat pads normal?
- Is the anterior humeral line normal?
- Is the radiocapitellar line normal?
- Are the ossification centers normal?
Step 1: Are the Fat Pads Normal?
The first step in evaluating a pediatric elbow radiograph is assessing the anterior and posterior fat pads. These fat pads lie within the joint capsule but outside the synovium and become displaced when an elbow effusion is present.
In a normal elbow, a small anterior fat pad may be visible on the lateral radiograph. However, when elevated away from the humerus, it produces the classic “sail sign,” which is considered abnormal. In contrast, a visible posterior fat pad is always abnormal and indicates a joint effusion (3).
 Figure 3
Figure 3
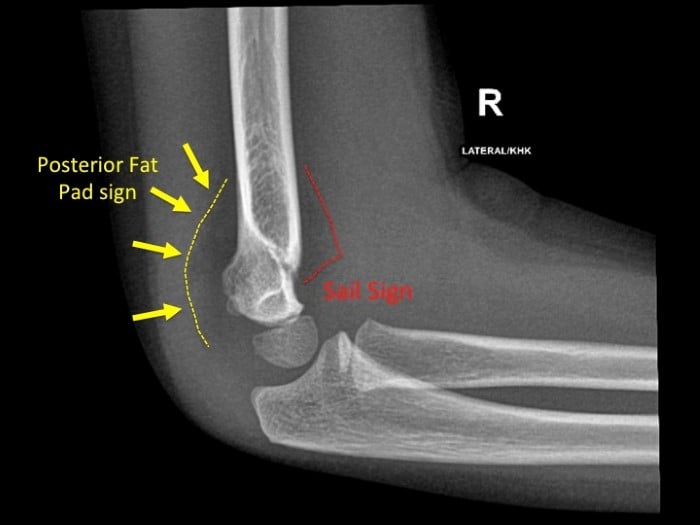 Figure 4
Figure 4
Case courtesy of Afra Alfalahi, Radiopaedia.org, rID: 54689
An elbow effusion in children should raise concern for an occult fracture, even if a fracture line is not immediately visible. Supracondylar fractures are among the most common associated injuries, although radial neck fractures, lateral condyle fractures, infection, and inflammatory conditions may also produce effusions (4).
Importantly, fat pad findings must always be interpreted in the appropriate clinical context. While trauma is the most common cause in the emergency department, septic arthritis or inflammatory arthropathies can produce similar radiographic appearances.
Step 2: Is the Anterior Humeral Line Normal?
The anterior humeral line is assessed on the lateral radiograph by drawing a line along the anterior cortex of the humerus. Normally, this line should intersect the middle third of the capitellum, or at minimum leave one-third of the capitellum anterior to the line. Of note, under the age of 4, it is normal for the line to intersect the anterior one-third of the capitellum.
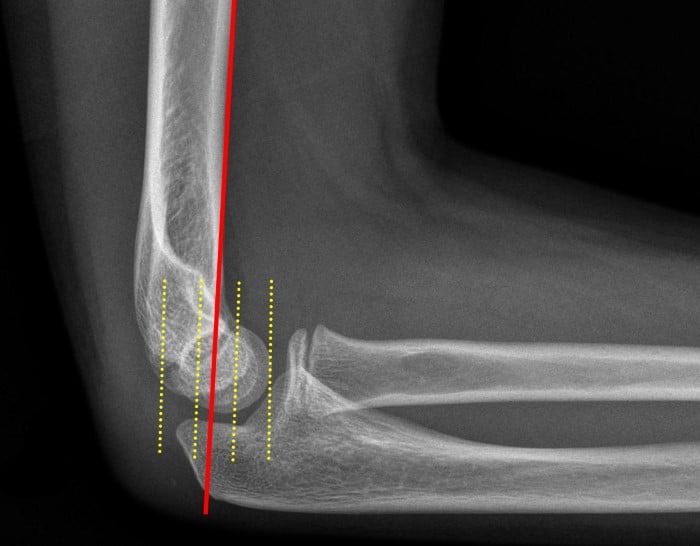 Figure 5
Figure 5
Case courtesy of Samir Benoudina, Radiopaedia.org, rID: 41167
(Normal Anterior Humeral Line)
Deviation of the capitellum posterior to this line suggests posterior displacement and is highly concerning for a supracondylar humerus fracture (5).
 Figure 6
Figure 6
Case courtesy of Leonardo Lustosa, Radiopaedia.org, rID: 97116
Supracondylar fractures are the most common elbow fractures in children and are particularly important because of their association with neurovascular injury. The brachial artery and median nerve are especially vulnerable. Delayed diagnosis may result in compartment syndrome, Volkmann ischemic contracture, or permanent neurologic deficits (6).
Clinical examination should therefore include careful documentation of:
- Radial and ulnar pulses
- Capillary refill
- Motor function of the median, radial, and ulnar nerves
- Sensory examination of the hand
Management depends on fracture displacement. Minimally displaced fractures may be immobilized in a posterior long-arm splint with close orthopedic follow-up, whereas significantly displaced fractures often require urgent orthopedic consultation and operative fixation (4).
Step 3: Is the Radiocapitellar Line Normal?
The radiocapitellar line is evaluated by drawing a line along the longitudinal axis of the radius through the radial neck and head. This line should intersect the capitellum on every radiographic view.
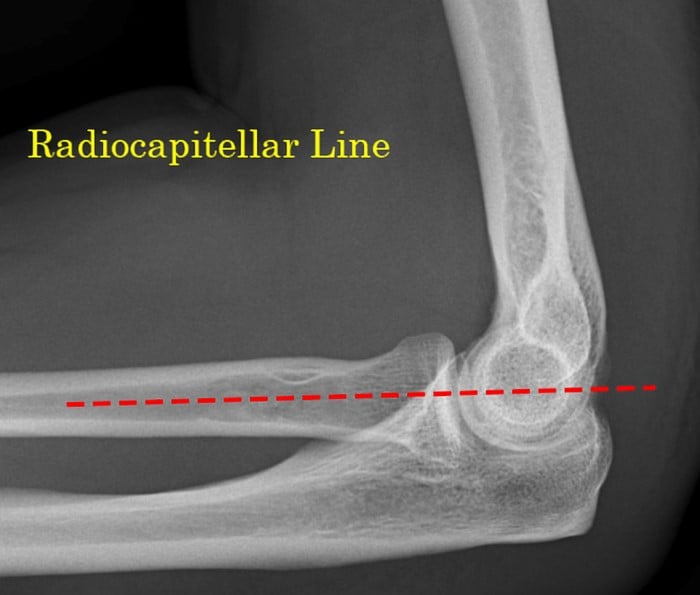 Figure 7
Figure 7
Case courtesy of Samir Benoudina, Radiopaedia.org, rID: 41196
Failure of the line to intersect the capitellum suggests radial head dislocation (7).
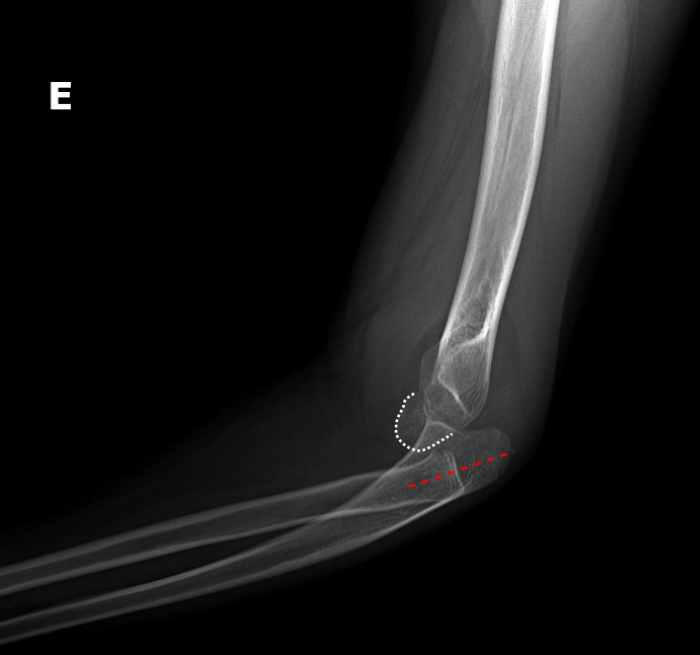 Figure 8
Figure 8
Case courtesy of Leonardo Lustosa, Radiopaedia.org, rID: 149776
(Associated ulnar bowing as well as radial head dislocation)
One important associated injury is the Monteggia fracture-dislocation, consisting of:
- Proximal or midshaft ulna fracture
- Radial head dislocation
Monteggia injuries are frequently missed in children because the ulna fracture may appear subtle or incomplete. Missing the radial head dislocation can result in chronic instability, pain, and decreased range of motion (8).
Because of this, emergency physicians should evaluate the radiocapitellar line on every pediatric elbow radiograph, regardless of the apparent injury.
Step 4: Are the Ossification Centers Normal?
Understanding pediatric elbow ossification centers is critical for distinguishing normal anatomy from fractures or avulsion injuries.
At birth, the distal humerus, proximal radius, and proximal ulna are largely cartilaginous and invisible on radiographs. Secondary ossification centers gradually appear throughout childhood in a predictable sequence commonly remembered using the mnemonic CRITOL:
|
Ossification Center |
Approximate Age of Appearance |
|
C-capitellum |
1 year |
|
R-radial head |
3 years |
|
I-internal (medial) epicondyle |
5 years |
|
T-trochlea |
7 years |
|
O-olecranon |
9 years |
|
L-lateral epicondyle |
11 years |
Table 1. CRITOL sequence of pediatric elbow ossification centers
While the exact age may vary, the sequence itself is generally reliable (9).
 Figure 9
Figure 9
Case courtesy of Leonardo Lustosa, Radiopaedia.org, rID: 207018
One especially important pearl is: “I before T.”
 Figure 10
Figure 10
Case courtesy of Andrew Dixon, Radiopaedia.org, rID: 9450
Looking at the above image, you can see that the ossification center sequence is disrupted.
The medial epicondyle (“Internal epicondyle”) should ossify before the trochlea. If the trochlea is visible but the medial epicondyle is absent, clinicians should suspect medial epicondyle avulsion with displacement into the joint space.
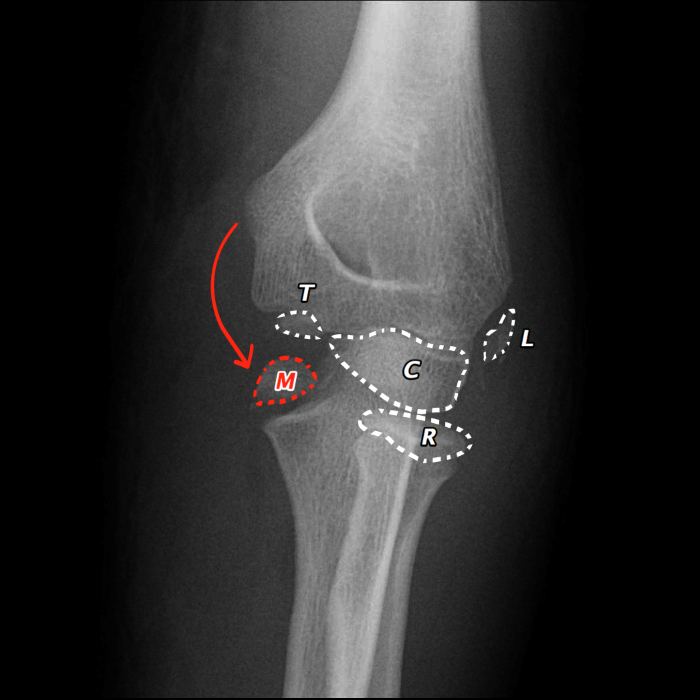 Figure 11
Figure 11
Case courtesy of Andrew Dixon, Radiopaedia.org, rID: 9450
Medial epicondyle avulsion injuries are commonly associated with elbow dislocations and valgus stress injuries. Because the fragment may become entrapped within the joint, missed injuries can result in chronic pain, instability, stiffness, and impaired function (10).
One challenge in pediatric elbow imaging is differentiating normal ossification centers from fracture fragments. Ossification centers are often irregular, fragmented, and incompletely corticated, which can mimic traumatic injury. Familiarity with expected developmental anatomy is therefore essential.
Lateral Condyle Fractures
Lateral condyle fractures are among the most commonly missed pediatric elbow fractures and deserve special attention.
These fractures often involve a substantial cartilaginous component of the distal humeral epiphysis that is not visible on radiographs. As a result, the true extent of injury may be underestimated on plain films. Functionally, these injuries behave similarly to Salter-Harris type IV fractures because they cross the physis into the articular surface (11).
 Figure 12
Figure 12
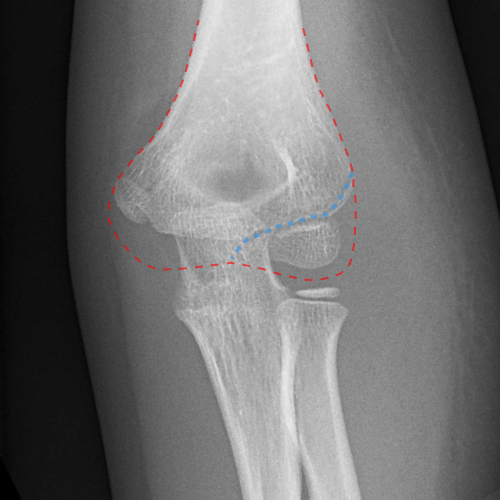
Figure 13
Case courtesy of Jeremy Jones, Radiopaedia.org, rID: 23652
(Dashed blue line represents fracture through lateral condyle)
Clinicians should maintain suspicion when:
- There is lateral elbow tenderness
- An elbow effusion is present
- Small metaphyseal fragments are visible
- Ossification centers appear asymmetric or displaced
An important association exists between olecranon fractures and lateral condyle fractures, and careful evaluation for concomitant injury is warranted.
Delayed or missed diagnosis can lead to:
- Nonunion
- Malunion
- Cubitus valgus deformity
- Chronic instability
- Loss of range of motion (12).
Because even minimally displaced fractures may require operative fixation, orthopedic follow-up is essential.
Nursemaid’s Elbow
Nursemaid’s elbow, or radial head subluxation, is one of the most common upper extremity injuries seen in young children.
It typically occurs in children between 1–3 years old after axial traction is applied to the arm, such as when a caregiver pulls upward on the child’s hand or forearm. This traction allows the radial head to partially slip beneath the annular ligament (13).
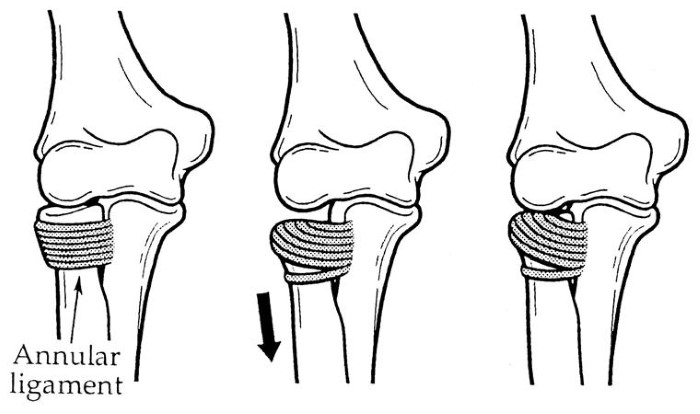 Figure 14 (15)
Figure 14 (15)
Patients classically present with:
- Refusal to use the affected arm
- Elbow held slightly flexed and pronated
- Minimal swelling or deformity
- Tenderness over the lateral elbow (13).
Because the diagnosis is primarily clinical, imaging is usually unnecessary when the history and examination are classic.
Reduction can generally be attempted immediately using either:
- Hyperpronation
- Supination with flexion
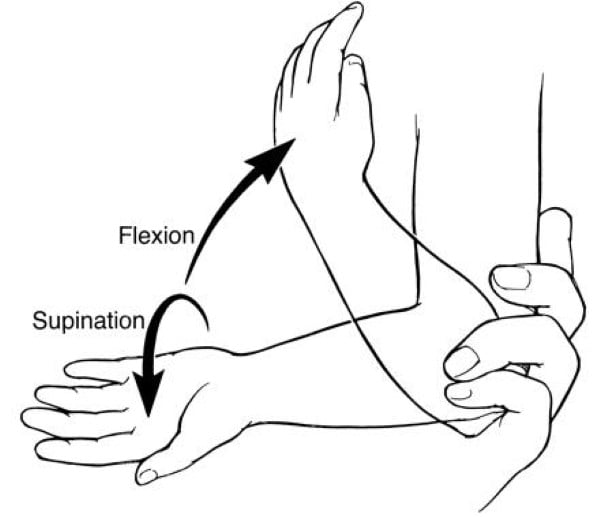 Figure 15
Figure 15
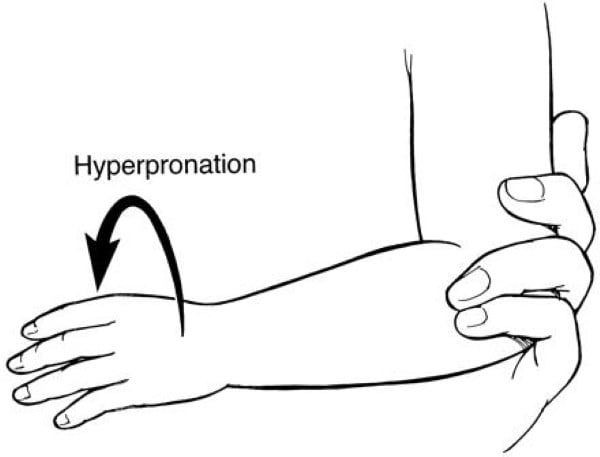 Figure 6 (15)
Figure 6 (15)
Both techniques are effective, although more recent literature suggests hyperpronation may have higher first-attempt success rates (14).
During reduction, clinicians may feel or hear a subtle “click” or “clunk” as the annular ligament repositions. Children typically begin using the arm normally within 15–30 minutes after successful reduction.
Interestingly, some nursemaid’s elbows spontaneously reduce during radiographic positioning, which occasionally explains a child who suddenly regains normal arm function after imaging.
Putting It All Together: A Stepwise Approach
Because pediatric elbow radiographs can initially appear overwhelming, maintaining a consistent search pattern is critical. A practical sequence includes:
- Assess for abnormal fat pads or effusion
- Evaluate the anterior humeral line
- Confirm the radiocapitellar line alignment
- Review the ossification centers using CRITOL
This systematic approach helps reduce missed injuries and improves confidence when interpreting pediatric elbow films in the emergency department.
Case Resolution
The 6-year-old patient demonstrates a marked anterior fat pad (“sail sign”), posterior fat pad sign and mild posterior displacement of the capitellum relative to the anterior humeral line, concerning for supracondylar humeral fracture.
 Figure 17
Figure 17
Case courtesy of Bálint Botz, Radiopaedia.org, rID: 61596
 Figure 18
Figure 18
Case courtesy of Bálint Botz, Radiopaedia.org, rID: 61596
The patient is placed in a posterior long-arm splint and orthopedic surgery is consulted. Neurovascular examination remains intact. He is discharged with close orthopedic follow-up and subsequently undergoes repeat imaging confirming a nondisplaced supracondylar fracture.
Summary and Recommendations
- Pediatric elbow injuries are challenging because of developmental anatomy and multiple ossification centers.
- A structured radiographic approach improves diagnostic accuracy:
- Fat pads
- Anterior humeral line
- Radiocapitellar line
- Ossification centers (CRITOL)
- Posterior fat pads are always abnormal and suggest an elbow effusion.
- Abnormal anterior humeral line alignment suggests supracondylar fracture.
- The radiocapitellar line should intersect the capitellum on all views.
- Knowledge of the CRITOL sequence helps differentiate normal ossification from fracture pathology.
- Medial epicondyle avulsions and lateral condyle fractures are commonly missed injuries.
- Nursemaid’s elbow is usually a clinical diagnosis and rarely requires imaging.
- Early recognition of pediatric elbow injuries helps prevent neurovascular compromise, growth disturbance, chronic instability, and long-term functional impairment.
References
- John S.D., Wherry K., Swischuk L.E., Phillips W.A. Improving detection of pediatric elbow fractures by understanding their mechanics. Radiographics. 1996;16:1443–1460. doi: 10.1148/radiographics.16.6.8946546.
- Bašković M, Pešorda D, Zaninović L, Hasandić D, Lohman Vuga K, Pogorelić Z. Management of Pediatric Elbow Fractures and Dislocations. Children (Basel). 2024 Jul 27;11(8):906. doi: 10.3390/children11080906. PMID: 39201841; PMCID: PMC11352739.
- Goswami G.K. The fat pad sign. Radiology. 2002;222:419–420. doi: 10.1148/radiol.2222000365.
- Hope N, Varacallo MA. Supracondylar Humerus Fractures. 2023 Aug 4. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan–. PMID: 32809768.
- Bašković M., Gregov A. Comprehensive Analysis of Pediatric Elbow Radiographic Lines and Angles. J. Orthop. Trauma. 2024;38:e55–e62. doi: 10.1097/BOT.0000000000002729.
- Hosseinzadeh P, Hayes CB. Compartment Syndrome in Children. Orthop Clin North Am. 2016 Jul;47(3):579-87. doi: 10.1016/j.ocl.2016.02.004. Epub 2016 Apr 22. PMID: 27241380.
- Jacoby S.M., Herman M.J., Morrison W.B., Osterman A.L. Pediatric elbow trauma: An orthopaedic perspective on the importance of radiographic interpretation. Semin. Musculoskelet. Radiol. 2007;11:48–56. doi: 10.1055/s-2007-984412.
- Zivanovic D., Marjanovic Z., Bojovic N., Djordjevic I., Zecevic M., Budic I. Neglected Monteggia Fractures in Children-A Retrospective Study. Children. 2022;9:1100. doi: 10.3390/children9081100.
- Cheng J.C., Wing-Man K., Shen W.Y., Yurianto H., Xia G., Lau J.T., Cheung A.Y. A new look at the sequential development of elbow-ossification centers in children. J. Pediatr. Orthop. 1998;18:161–167. doi: 10.1097/01241398-199803000-00006.
- Pathy R, Dodwell ER. Medial epicondyle fractures in children. Curr Opin Pediatr. 2015 Feb;27(1):58-66. doi: 10.1097/MOP.0000000000000181. PMID: 25564187.
- Milch H. Fractures and fracture dislocations of the humeral condyles. J. Trauma. 1964;4:592–607. doi: 10.1097/00005373-196409000-00004.
- Lam KY, Mahadev A. Combined lateral condyle mass and olecranon fractures: A proposed treatment algorithm and surgical technique. J Orthop Surg (Hong Kong). 2019 May-Aug;27(2):2309499019837146. doi: 10.1177/2309499019837146. PMID: 30894060.
- Paluch LK. Nursemaid's elbow: Radial head subluxation injuries in children. JAAPA. 2024 Jun 1;37(6):18-21. doi: 10.1097/01.JAA.0000000000000025. Epub 2024 May 28. PMID: 38747889.
- Ulici A, Herdea A, Carp M, Nahoi CA, Tevanov I. Nursemaid's Elbow - Supination-flexion Technique Versus Hyperpronation/forced Pronation: Randomized Clinical Study. Indian J Orthop. 2019 Jan-Feb;53(1):117-121. doi: 10.4103/ortho.IJOrtho_442_17. PMID: 30905991; PMCID: PMC6394198.
- Nursemaid’s Elbow. Note. From "Nursemaids Elbow," by Orthobullets, 2022. Orthobullets (orthobullets.com). Reprinted with permission.


