
No Leg to Stand On
A 17 Year-old Football Player with Bilateral Leg Fractures
Affiliation:
- Albany Medical Center
- Albany, NY 12208
All Authors:
- Stewart William Lee, MD
- Yvonne Chow, MD
Case Report
Patient is a 17 year old high school American football player at the running back position who presents with distal lower extremity pain after being tackled during a routine football play. Following the tackle, the patient felt immediate pain to his right distal lower extremity. He attempted to stand but found his right lower extremity to be deformed laterally at the mid shin. The right leg was splinted on site by first responders and the patient was then transported to the Emergency Department for further evaluation. While in route, the EMS secondary assessment revealed swelling and tenderness to palpation of patient’s left ankle. This ankle was then also splinted. No other injuries were noted. Patient is otherwise healthy and has no pertinent medical history and stable vital signs throughout. Past surgical history of tonsillectomy.
On presentation to the emergency department, the patient’s physical exam revealed obvious right open mid shaft tibia/fibula fracture with soft compartments with 1 cm laceration overlying bone. Left ankle was swollen and tender. Both lower extremities were neurovascularly intact.
The patient had both lower extremities splinted in the emergency department by orthopedics and was given antibiotics and pain control. He was taken to surgery early the next morning for open reduction and internal fixation of the left trimalleolar fracture, intramedullary rodding of the right tibia, and irrigation and debridement of the open fracture. Following surgery, he was observed in PACU to have increased right leg pain, with firmness of the anterior and lateral compartments. Compartment pressure measurements were found to be greater than 50 mmHg. He was diagnosed with compartment syndrome and was taken back to the operating room for right lower extremity fasciotomy. Fasciotomy incisions were closed 3 days later. Following a 9-day inpatient stay, he was transferred to an inpatient rehabilitation facility for further physical and occupational therapy.
The patient is currently 10 months out from the injuries and continues to convalesce with physical and occupational therapy, still requiring ambulation with a walker. Rehabilitation for this patient was complicated by the bilateral nature of his injuries. Immediate weightbearing on his right leg following intramedullary fixation was difficult due to his left leg being nonweightbearing for the weeks following the ORIF of the left trimalleolar fracture. He has suffered from recurrent staph infection beginning 2 months out from initial surgery requiring multiple courses of antibiotics and long term daptomycin treatment.

X-Ray Results
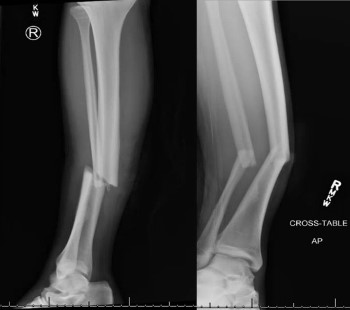
Right Tib-Fib Xray: Right angulated mid-shaft fracture of tibia and fibula
Left Ankle Xray: Left trimalleolar fracture with oblique fractures of posterior tibia and distal fibula with posterior-lateral displacement of fragments.
Discussion
Mid-shaft tibia/fibula fractures and trimalleolar fractures are rare but severe sports injuries. Acute mid-shaft tibial fractures with concomitant fibular fractures have the longest return-to-sports timing of all sports fractures (41-55 weeks), but with relatively good outcomes. Up to 92% of athletes can return to sports after surgical treatment such as intramedullary nailing, open reduction and internal fixation, and external fixation. However, complications can occur, including compartment syndrome, infection, nonunion, DVT, fat embolism and persistent knee pain. [Robertson, 2016] [Court-Brown, 2006]
Tibial diaphyseal fractures are the most common cause for compartment syndrome, which involves elevated muscle compartmental pressures that reduce blood flow and result in ischemia of muscle tissue. This complication occurs in 4.3-7% of closed and 3.3%-9.1% of open tibial fractures. [Court-Brown, 2006] Treatment involves prompt fasciotomy. Risk factors include young male athletes involved in a high mechanism long bone injury and is hallmarked by pain with active and passive range of motion that is out of proportion to exam, along with sensory deficit and loss of distal pulses. Complication rate increases with delay in diagnosis and treatment and include muscle weakness and contractures, sensory loss, infection, and fracture nonunion. [Court-Brown, 2006] [Tintinalli, 2016]
Trimalleolar fractures represent only 7% of all ankle fractures, but such injuries can be devastating. The majority are unstable and require early surgical management. Only about 30% of athletes who suffer a trimalleolar fracture return to their pre-injury level of sports, and 25% of athletes are unable to return to sports at all. Patients must be counseled about long-term residual pain, stiffness, and swelling for realistic recovery expectations. [Hong, 2014] [Robertson, 2015] Together, this patient suffered two of the most severe orthopedic lower extremity fractures in sports during a single football play.
This case also highlights the importance of a thorough secondary assessment. When an injury requires a high mechanism of injury, such as a mid-shaft tib-fib fracture, concomitant injuries may also be present. A full head-to-toe physical exam is necessary and the examiner must be cautious not to be distracted from other injuries by the obvious injury.
References:
- Hong CC, Nashi N, Prosad RS, Tan KJ: Impact of Trimalleolar Ankle Fractures: How do Patients Fare Post-Operatively. Foot Ankle Surg. 2014 Mar; 20: 48-51
- Robertson GA, Wood AM: Return to Sport After Tibial Shaft Fractures: A Systematic Review. Sports Health. 2016 Jul; 324-30
- Robertson G, Wood A. Fractures in sport: Optimising their management and outcome. World J Orthop. 2015 Dec 18; 6(11): 850–863
- Court-Brown CM, McQueen MM, Tornetta PI. Trauma. Orthopaedic Surgery Essentials Series. Vol. 1st ed. Philadelphia: Lippincott Williams & Wilkins; 2006.
- Tintinalli JE, Stapczynski JS, et al. Tintinalli's Emergency Medicine: A Comprehensive Study Guide. Eighth edition. New York: McGraw-Hill Education, 2016


