Second Impact Syndrome (SIS)
By Kalvis Hornburg, MD
In 2019, a 17 year old Canadian rugby player named Rowan Stringer was caught in a high tackle. She sat up, then lost consciousness. EMS, who arrived within just minutes, found her with fixed and dilated pupils and a GCS of 3. While in the hospital, despite aggressive resuscitation and herniation management (including a decompressive craniotomy), she unfortunately passed four days later due to severe cerebral edema. A later inquest revealed two recent head injuries and that she had been complaining about concussion symptoms in texts to friends. Ultimately, her death was attributed to Second Impact Syndrome 1.
What is Second Impact Syndrome (SIS)? It is an incredibly rare but potentially fatal condition that occurs when a patient sustains a second head injury before fully recovering from an initial concussion. It’s characterized by rapid cerebral swelling, brain herniation, and often death 2. Despite its severity, the prevalence of SIS remains poorly understood due to limited epidemiological data and the rarity of documented cases, with some even debating its existence as a unique syndrome.
The underlying pathophysiology is thought to be related to cerebral autoregulation failure. Essentially, after the first concussion, the brain goes into a hypermetabolic recovery state with alterations to normal cerebral blood flow and electrolyte concentrations 3. In this vulnerable state, a second head injury can lead to rapid cerebral edema and even death within minutes, usually via uncal herniation. This is thought to be due to the loss of some of these normal regulatory pathways (control of blood flow and electrolyte gradients). So, while normal traumatic brain injury patients with similar mechanisms of injury may be able to compensate for some time, these vulnerable brains can succumb rapidly.
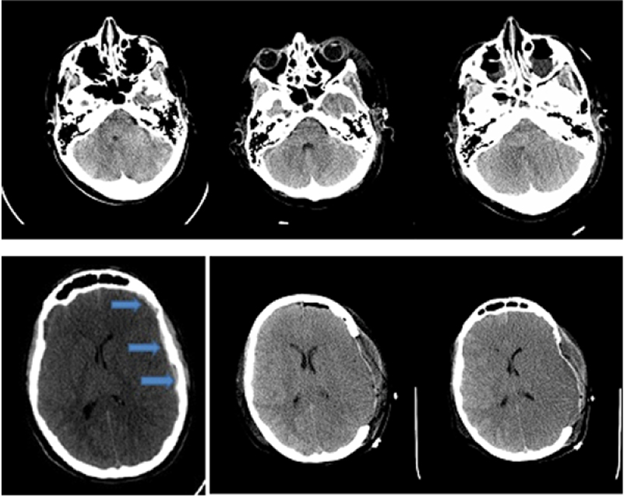 Rowan Stringer’s CT Non-Con at 2h post-injury (1st column), 2d post-injury s/p craniotomy (2nd column), and 3d post-injury (3rd column) 1
Rowan Stringer’s CT Non-Con at 2h post-injury (1st column), 2d post-injury s/p craniotomy (2nd column), and 3d post-injury (3rd column) 1
Very little data is available to get a sense of the true prevalence of this condition. There are fewer than 20 actual documented cases in the literature 2, and limited epidemiologic data means it’s not even clear how many patients or athletes develop a second brain injury before recovering from an initial concussion. Some analyses suggest the true prevalence is far higher in the setting of missed or alternative diagnoses 4.
Treatment remains primarily focused on prevention. Good concussion protocols with gradual return to play protocols are the mainstay. Education can also go a long way in discouraging young athletes from coming back before they are recovered, or even encourage them to be more forthcoming about initial concussion symptoms 5.
Identification/Screening:
- Symptoms are often myriad and are difficult to pick up on. Any neurologic symptoms of any kind, as well as high-risk mechanisms of injury should raise red flags 6. Symptoms can include headache, confusion, dizziness, imbalance, nausea or vomiting, repetitive questioning, visual changes, and discoordination
- Standardized assessments like the SCAT5 or Child SCAT5 7 can help further elicit more subtle symptoms but are more intensive and require a medical professional. It includes the following evaluations that can be started immediately upon injury and continued later:
- On-Field: Symptom assessment, Memory assessment (Maddock questions), GCS exam, C-spine exam
- Off-Field: Cognitive screening, Neurologic screening, Balance exam, Concentration testing, and a delayed recall test.
Management + Education:
- Protocolized return to play can be helpful for establishing set rest periods and clearance evaluations. They can be sport specific based on risk of re-injury, and can help prevent premature return (the primary risk factor for SIS). Pre-established protocols vary widely across sports and organizations, however, which highlights the importance of consensus among professionals and teams before an injury occurs 8.
- Emphasis on education of athletes, team personnel, and medical professionals on symptom identification as well as highlighting the ramifications to athlete health can further improve practice. An example includes the CATT (Concussion Awareness and Training Tool) educational modules.
- Building a culture of reporting and emphasizing health as well as identifying barriers to identification and treatment, while somewhat nebulous, is an important element to preventing catastrophes like SIS 9.
In the case of an acute event of SIS, the priority is on stabilization, including airway management, hyperosmolar therapy, seizure management, and transfer to a facility with appropriate neurosurgical services.
Citations:
- Tator C, Starkes J, Dolansky G, Quet J, Michaud J, Vassilyadi M. Fatal second impact syndrome in rowan stringer, a 17-year-old rugby player. Can J Neurol Sci. 2019;46(3):351-354.
- Dessy, A. M., Rasouli, J., & Choudhri, T. F. (2015). Second Impact Syndrome: A Rare, Devastating Consequence of Repetitive Head Injuries. Neurosurgery Quarterly, 25(3), 423-426. https://doi.org/10.1097/WNQ.0000000000000085
- Bey T, Ostick B. Second impact syndrome. West J Emerg Med. 2009;10(1):6-10.
- Stovitz SD, Weseman JD, Hooks M, Schmidt RJ, Koffel J, Patricios JS. What Definition Is Used to Describe Second Impact Syndrome in Sports? A Systematic and Critical Review. Current Sports Medicine Reports. 2017;16(1):50-55. doi:10.1249/JSR.0000000000000326
- May T, Foris LA, Donnally CJ. Second Impact Syndrome. StatPearls Publishing; 2017. https://pubmed.ncbi.nlm.nih.gov/28846316/
- Tomkinson CB, Weston E, Batt AM. A Review of Concussion Recognition, Assessment and Management for Paramedics. Published online January 1, 2017. https://first.fanshawec.ca/cgi/viewcontent.cgi?article=1014&context=fhcsps_publicsafety_facultystaffpublications
- Echemendia RJ, Meeuwisse W, McCrory P, et al. The Sport Concussion Assessment Tool 5th Edition (SCAT5): Background and rationale. Br J Sports Med. 2017;51(11):848-850. doi:10.1136/bjsports-2017-097506
- Prock M, O'Sullivan DM, Tiernan S. Comparing return to play protocols after sports-related concussion among international sporting organisations. Phys Sportsmed. 2024;52(5):421-431. doi:10.1080/00913847.2024.2344432
- Kneavel M, Ernst W, Brandsma L. Collegiate athletes' perceptions of the culture of concussion reporting. J Am Coll Health. 2021;69(4):435-443. doi:10.1080/07448481.2019.1679816