

This week, I’ve called in a reliever—a 6’ 3” right-hander with a nasty changeup and, better yet, someone who has a solid grasp of state issues and regulatory policy. I can think of no one better than Mr. Adam Krushinskie to explain the ins and outs of the new federally mandated crisis number, 988, which is supposed to be implemented across the country starting this Saturday, July 16th. Adam is ACEP’s Reimbursement Manager. If you ever wonder how ACEP manages to stop bad insurer policies (like this one) before it negatively impacts the work you do every day, Adam has your back. He also works closely on balance billing/out-of-network legislation and is a go-to resource at the College on Medicaid and managed care issues.
So, without further ado, I’ll let Adam take it away…
Thank you, Jeffrey! As many of you know, our country is facing a mental health crisis. The rate of suicide has outpaced deaths from motor vehicle accidents in the US for over a decade. Let that statistic sink in for a moment – nearly half a million lives lost because many Americans experiencing a mental health crisis feel they have no one to talk to and nowhere to turn for help.
As Jeffrey stated above, the 988 crisis hotline will be available starting July 16th to all landline and cell phone users, providing a single three-digit number to access a network of local and state funded crisis centers. 988 callers who are suicidal or experiencing a mental health crisis will be routed to the National Suicide Prevention Lifeline and connected to a crisis counselor where they may receive crisis counseling, resources, and in some cases and where available, a mobile crisis unit may be dispatched.
While there is no doubt that 988 will save lives, there is a lot of concern with who will pay for it and how the patchwork of local and state crisis centers will handle the expected call volumes. 988 is the first major change in generations for Americans seeking help in an emergency. Our more senior readers may remember November 1967 when 911 was first established as the universal emergency number. Implementation and awareness take time. It took until 1987 – 20 years – for 50% of the US population to have access to 911. State and local authorities know how to stick the landing with 988 from that experience – they just need the resources to pull it off.
According to a recent Rand Corp. report, more than half of public health officials said they felt unprepared and without necessary financing for staffing or infrastructure to handle the rollout. In a time when many states have a surplus due to increased income and sales tax revenues, legislators in 29 states have done little to nothing to support 988. Much of this has to do with 988’s consideration as an unfunded federal mandate; however, the ensuing debates in state houses has uncovered decades of underfunding for mental health services.
- People experiencing a mental health, substance use or suicide crisis need:
- Someone to call
- Someone to respond
- Somewhere to go
What can you all as emergency physicians do to help? One in five Americans experience mental illness each year. You continue to roll up your sleeves daily and help in the darkest hour. 988 will inevitably increase patient volume as the emergency department (ED) is the first place people will turn during a crisis. 24/7 local crisis call centers, mobile crisis teams, and crisis stabilization options will integrate EMS and the ED into the National Suicide Prevention Lifeline—so 988 callers actually receive the help they need. What is needed most right now are state and local laws and regulations that change the way communities respond to citizens in a mental health crisis.
Congress passed the 988 National Suicide Hotline Designation Act establishing 988 into law and directing states to create statewide coordinated crisis services systems with adequate and stable funding, in October 2020. It is now up to the states to carry the water. The National Alliance on Mental Illness (NAMI) has created model legislation that includes a new funding mechanism for states to create a monthly fee on all phone lines—similar to how communities fund 911—to ensure that 988 funding is sustainable and that emergency services will not experience funding gaps. To protect against fee diversion, the model bill requires 988 fees to be deposited in a trust fund that can only be used to support 988. Progress has been slow, with only eight states having enacted 988 infrastructure in time for the July 16th rollout.
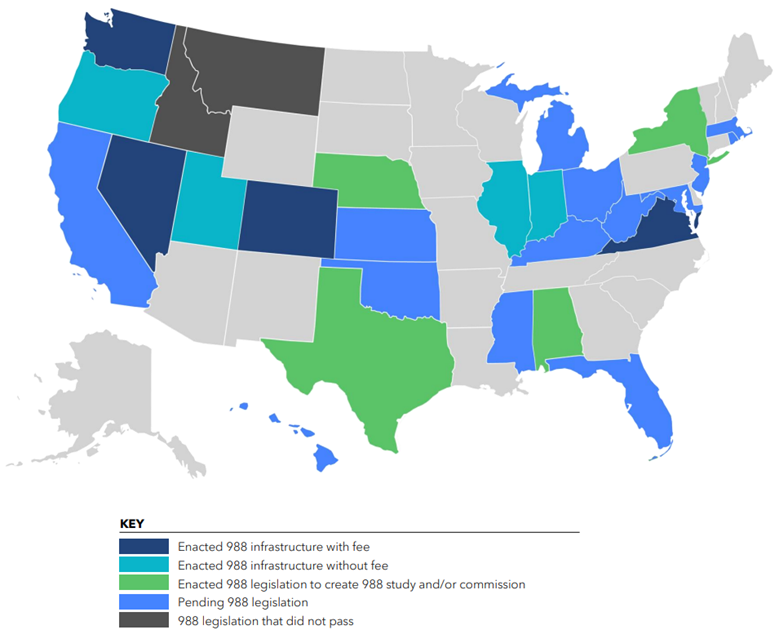
Thirty-three states have yet to pass legislation that will support the crisis centers that will begin answering calls this weekend. The lack of progress on funding discourages callers in crisis to call again the next time they are experiencing a crisis and could lead to frustrated callers on hold hanging up the phone and attempting suicide. Worse yet, the majority of call centers are only able to answer 80 percent of the mental health crisis calls that come in every day. The lack of funds prevent centers from de-escalating life-threatening situations in which people otherwise might have had to call 911, go to the ED, or ultimately die by suicide.
Many states who have done little or nothing to implement 988 have a largely rural population. Suicide death rates in 2020 were highest among American Indian and Alaska Native people, males, and people who live in rural areas. Many of these same states have been dealing with issues such as opioid abuse and high unemployment from the ongoing “brain drain” epidemic due to a shift away from a manufacturing-based economy—both of which increase the chances of suicide.
Urban areas are seeing similar increases. Suicide deaths are increasing fastest among people of color, as well as younger individuals. A persistent underdiagnosis of mental health conditions, structural barriers to care, stereotypes associated with poor mental health, racism and discrimination, and disparities in the use of mental health services are all contributing to rising suicide rates among people of color.
While some states that have done very little to support 988 are hoping for the feds to intervene once the rollout does not go as smoothly as planned, others have taken an indirect approach to support mental health crisis services. For example, last year, South Carolina passed the Student Identification Card Suicide Prevention Act, which required the National Suicide Prevention Lifeline to be printed on the student identification cards of students from grade seven through the university level. Within 24 hours of the start of the school year, the life of a child was saved.
Transforming our crisis systems will take more than a patchwork of approaches – we need 988 to be implemented to strengthen the national network of providers. The National Association of State Mental Health Program Directors has created a playbook for states to follow. The Substance Abuse and Mental Health Services Administration (SAMHSA) has also released a comprehensive FAQ that answers a lot of the most basic questions about how 988 will work. One interesting aspect of the system is that not only can individuals call 988; they can also text or chat 988 if they choose not to speak over the phone.
Suicide has affected our lives in ways we can never ignore: 33% of people say they know someone who has died by suicide, while 9% say they have attempted suicide. However, we also know that when someone has a person to talk to, suicide rates decrease significantly. Now is the time to give Americans a trained person to talk to 24/7 when they need it.
So, how will the introduction of this number affect you and the EDs where you work? This is a great question that unfortunately does not have a clear answer at this time. NAMI believes that a crisis standard of care in every community that provides a continuum of crisis services will alleviate some of the revolving door of ED visits. However, increasing visibility of crisis services through 988 and the potential to remove some of the stigma associated with reaching out for help in an emergency could lead to higher patient volume in the ED. Some individuals in crisis will need short-term observation and stabilization. You also may need help identifying additional treatment needs and providing a “warm hand-off” to follow-up care, from peer supports and outpatient services to more intensive services, such as hospitalization. We will need to pay attention to ED and inpatient data to determine if an increased demand for services is resulting in increased patient boarding or delays in accessing the continuum of mental health care.
For now, please take a moment and read what your state is doing to implement 988. Chances are that not much has been done. Now is the time to talk to your state legislators about ways in which model legislation can be introduced during the next legislative session in your state.
Found below are some resources that ACEP has put together to help you understand how this new lifeline will potentially affect you, your patients, pre-hospital care, and overall ED utilization. Please feel free to reach out to me, Adam Krushinskie, at akrushinskie@acep.org, or others on the ACEP team with any questions. I’m sure the road ahead will be bumpy, but our ultimate hope is that this new number will help people get the most appropriate care in their greatest time of need.
Until next week, this is Adam (and Jeffrey) saying, enjoying reading regs with your eggs!
ACEP Resources on 988:
Webinar: To better understand how this change affects emergency medicine, watch the on-demand webinar featuring Emmy Betz, MD, MPH, a leading suicide prevention researcher; John Draper, PhD, executive director of the National Suicide Prevention Lifeline; and Tony Ng, MD, chair of the Coalition of Psychiatric Emergencies.
Podcast: ACEP Frontline host Dr. Ryan Stanton talks with John Draper, executive direction of the Lifeline, about the implications of this new lifeline and how it could affect emergency medicine.
Map: See how your state is preparing for the launch of 988.
Playbook: This SAMHSA resource helps assess and improve your institution’s readiness for the launch of this new lifeline.



