Recommendations for the use and cleaning of non-medical respirators in Emergency Medicine during the COVID-19 pandemic
Howard Mell, MD, MPH, FACEP
Christopher Guyer, MD, FACEP
Mary-J Thompson, CSP, CHMM
Other recommended reports:
National Academy of Science Reusable Elastomeric Respirators in Health Care: Considerations for Routine and Surge Use
CDC Elastomeric and Powered-Air Purifying Respirators in US Healthcare
Procedures commonly encountered in the practice of Emergency Medicine that are believed to generate aerosols and droplets as a source of respiratory pathogens include cardiopulmonary resuscitation, positive pressure ventilation (BiPAP and CPAP), endotracheal intubation, extubation, airway suction, high frequency oscillatory ventilation, tracheostomy, chest physiotherapy, nebulizer treatment, sputum induction, and bronchoscopy. These procedures are known to stimulate coughing and to promote the generation of aerosols, however their risk of infection transmission is not known with certainty1. Coughing, sneezing, talking and breathing also generate infectious respiratory aerosols.
Limited research exists on transmission routes of SARS-CoV-2. Transmission likely occurs via multiple routes. In a recent JAMA study SARS-CoV-2 was detected in upper and lower respiratory tract samples as well as in stool and blood samples2. A recent study also showed that SARS-CoV-2 remained viable in aerosols for 3 hours under experimental conditions3.
In a handbook provided by the First Affiliated Hospital of Zhejiang University, the authors describe technical strategies for addressing issues in the fight against COVID-19 based on experience in China. They offer three levels of suggested protection for staff in healthcare facilities and specifically state that "all staff working in the emergency department ... must upgrade their surgical masks to medical protective masks (N95) based on Level I protection." Suggested Level 1 protection includes a disposable surgical cap, disposable surgical mask, work uniform, disposable latex gloves or/and disposable isolation clothing if necessary4.
Current CDC recommendations for healthcare workers caring for patients with known or suspected COVID-19 include the use of a respirator or facemask (if a respirator is not available) before entry into the patient room or care area. Recommendations also include the use of eye protection (goggles or a face shield that covers the front and sides of the face), gloves and gowns. https://www.cdc.gov/coronavirus/2019-ncov/infection-control/control-recommendations.html
To minimize their risk of exposure, healthcare workers would benefit from the use of a respirator mask. The most commonly used mask in clinical settings is the N95 mask. Individuals working in Emergency Medicine settings are familiar with their use and perform annual training and fit testing with available devices. In the current healthcare environment, N95 masks are in short supply and the use of alternatives has been suggested.
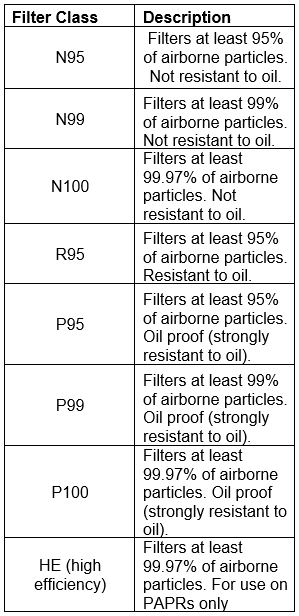
The “N” designator of a N95 mask refers to the mask’s resistance to oil, not a medical designation. 95 refers to the percent of particulate matter filtered. Thus, a P100 mask (oil proof and filtering 99.97% of all particulates) is superior to an N95. There are masks with P95 and P100 filters designed for long term wear in industrial settings with replaceable cartridges. https://www.osha.gov/video/respiratory_protection/resptypes_transcript.html and https://ebolapreparedness.org/n95-vs-p95-vs-r95-respirator-masks/
Table 1. NIOSH Filter Classes
The Food and Drug Administration (FDA) has issued an Emergency Use Authorization (EUA) for emergency use of: (1) all disposable filtering facepiece respirators (FFRs) approved by the National Institute for Occupational Safety and Health (NIOSH), in accordance with 42 CFR Part 84, as non-powered air-purifying particulate FFRs for use in healthcare settings by healthcare personnel (HCP) to prevent wearer exposure to pathogenic biological airborne particulates during FFR shortages resulting from the Coronavirus Disease 2019 (COVID-19) outbreak. https://www.fda.gov/media/135763/download
A list of NIOSH approved filtering facepiece respirators (FFRs), as well as extensive instructions for determining if a respirator meets the requirements can be found here: https://www.cdc.gov/niosh/npptl/topics/respirators/disp_part/default.html
The NIOSH states that the manufacturers’ recommended procedures for performing a user seal check can be included in the donning procedures and/or user instructions as alternatives to the OSHA-specified procedures under the respiratory protection standard (See 29 CFR 1910.134 Appendix B-1). NIOSH does not evaluate the efficacy and reliability of any user seal check procedures, but OSHA will accept the manufacturer’s recommended procedures if the employer demonstrates those procedures are equally effective as those identified in the standard. In short, follow the directions included with your mask.
Using these respirators raises an issue of how best to don, doff and clean them and, in some cases, guidance is needed regarding changing disposable filters. Manufacturers instructions suggest the filter replacement interval with the typical recommendation for replacement being after 40 hours or 30 days of use. Donning and doffing a respirator should be performed according to the manufacturers recommendations for the specific product being used. Since the respirator itself may be contaminated, healthcare workers should handle it with gloves after use and use appropriate personal protective equipment during the cleaning and disinfecting process5.
Cleaning and disinfecting non-disposable filtering facepiece respirators in healthcare applications is another new challenge. The CDC recommends disinfecting equipment and surfaces potentially contaminated by coronaviruses. However, research during the H1N1 pandemic indicated that cleaning respirators was as effective as disinfection at removing virus from respirator surfaces.6
3M recommends using sodium hypochlorite at a free chlorine concentration of 5,000 ppm to clean their reusable respirator facepieces. This is effective after a 1-minute contact time. https://multimedia.3m.com/mws/media/1793959O/cleaning-and-disinfecting-3m-reusable-respirators-following-potential-exposure-to-coronaviruses.pdf
There is no reason to expect that these guidelines would be significantly different for other respirators.
They suggest:
During coronavirus outbreaks, some healthcare organizations may assign reusable elastomeric facepieces to workers providing care for patients with suspected cases of coronavirus. This document contains considerations related to cleaning and disinfecting facepieces that will be used again after potential exposure to coronaviruses. The 2008 U.S. CDC publication https://www.cdc.gov/infectioncontrol/pdf/guidelines/disinfection-guidelines-H.pdf (updated May 2019)7 includes information on disinfecting equipment and surfaces potentially contaminated by coronaviruses. The US CDC investigated many chemicals and cited several chemical germicides as being effective for coronaviruses, when used as indicated in the product user instructions. One of these chemicals can be used to clean 3M reusable respirator facepieces per the 3M product User Instructions and those included in this document:
Your facility should review this information thoroughly prior to selecting this disinfecting product for your equipment and specific application. Follow the hygiene and infection control practices established by your employer for the targeted organisms, including coronaviruses. Please note that 3M has not evaluated the effectiveness of this agent with regards to inactivating viruses on 3M equipment. Please always refer to the latest information from trusted sources such as the World Health Organization (WHO), the US Centers for Disease Control and Prevention (US CDC), the US Occupational Safety and Health Administration (OSHA) and the European Centres for Disease Prevention and Control (ECDC) regarding selection, use, maintenance and cleaning of personal protective equipment. Note that respirator facepiece components may become damaged over time with prolonged or extended use of disinfecting products. As discussed in the product User Instructions, users must inspect their respirator following each disinfecting cycle and prior to re-use. If you discover any signs of damage, remove the facepiece from service and either discard and replace or repair as appropriate, following the guidance in the product User Instructions.
Cleaning, Sanitizing and/or Disinfecting Half and Full Facepieces
1) Cleaning is recommended after each use. Nitrile or vinyl gloves should be worn during cleaning as well as other personal protective equipment (PPE) as indicated.
2) Remove and discard any filters or cartridges (edit: that are visibly contaminated or soiled). Facepiece may be further disassembled as necessary.
3) Inspect facepiece per the User Instructions to identify any damage or excessive wear. Repair or replace facepiece as necessary.
4) Clean facepiece (excluding filters or cartridges) by immersing it in a warm cleaning solution, water temperature not to exceed 120 °F (49 °C), and scrub with soft brush until clean. Add neutral detergent if necessary. Do not use cleaners containing lanolin or other oils
5) Disinfect by soaking the facepiece according to the user instructions for the selected disinfectant, including usability, application and contact time.
Effective after a 1-minute contact time:
• Sodium hypochlorite (at a free chlorine concentration of 5,000 ppm)
6) Rinse thoroughly with fresh warm water.
7) Air dry in non-contaminated area.
8) Inspect and reassemble respirator as described in the User Instructions
A study in 2015 suggested in a feasibility study that healthcare workers following a standard operating procedure without specific training or guidance made no errors when disinfecting masks8.
Precedent exists for the use of reusable respirators. During the H5N1 avian influenza pandemic the University of Maryland Medical Center successfully deployed reusable elastomeric respirators to high risk units and staff when it was apparent that the supply chain would not be able to provide sufficient PPE for their staff9.
References
- Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(4):e35797. doi:10.1371/journal.pone.0035797
- Wang W, Xu Y, Gao R, et al. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA. Published online March 11, 2020. doi:10.1001/jama.2020.3786
- Vvan Doremalen N, Morris D, Holbrook M. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1 | NEJM. New England Journal of Medicine. https://www.nejm.org/doi/full/10.1056/NEJMc2004973?query=featured_home&utm_source=newsletter&utm_medium=email&utm_campaign=newsletter_axiosvitals&stream=top. Published 2020. Accessed March 23, 2020.
- Handbook of COVID-19 Prevention and Treatment. https://covid-19.alibabacloud.com/. Published March, 2020. Accessed March 23, 2020.
- National Academies of Sciences, Engineering, and Medicine. 2019. Reusable Elastomeric Respirators in Health Care: Considerations for Routine and Surge Use. Washington, DC: The National Academies Press. https://doi.org/10.17226/25275.
- Lawrence C, Harnish DA, Sandoval-Powers M, Mills D, Bergman M, Heimbuch BK. Assessment of half-mask elastomeric respirator and powered air-purifying respirator reprocessing for an influenza pandemic. Am J Infect Control. 2017;45(12):1324–1330. doi:10.1016/j.ajic.2017.06.034
- Rutala, WA. CDC. Guideline for Disinfection and Sterilization in Healthcare Facilities. 2008.
- Bessesen M, Adams J, Radonovich L, Anderson J. Disinfection of reusable elastomeric respirators by health care workers: A feasibility study and development of standard operating procedures. Am J Infect Control. 2015;43(6):629-634. doi:10.1016/j.ajic.2015.02.009
- Chang J. Use of elastomeric respirators in clinical practice: The UMMC experience. Washington, DC: 2018. Presentation at the March 22, 2018, public meeting of the National Academies of Sciences, Engineering, and Medicine Committee on the Use of Elastomeric Respirators in Health Care.