
I’ve been posting about the hydroxychloroquine literature since the beginning of this pandemic. The message at the outset was pretty clear: “there is no reason to be using chloroquine at this point.” I have updated that primary post a number of times and the message has remained unchanged. There was never any good evidence that hydroxychloroquine helped patients with COVID, and there was never any good reason to be prescribing it clinically.
With the publication of interim results from the SOLIDARITY trial, there is no longer any doubt. (Pan 2020) Hydroxychloroquine doesn’t help. In fact, it looks like it probably hurts, and the overzealous adoption of an unproven medication may have caused a lot of unnecessary deaths early in this pandemic. For the most part, the debate around hydroxychloroquine has died down, but this data should serve as an important reminder of the harms of ignoring the scientific process, and the potential ongoing harms from other unproven medications that we continue to use for COVID-19 patients. (Carley 2020)
The SOLIDARITY trial
The SOLIDARITY trial is a large, adaptive-design, multi-national trial that is looking at a number of different medications in the treatment of inpatients with COVID-19. The initial drugs under investigation were remdesivir, hydroxychloroquine, lopinavir-ritonavir, and interferon-β1a. At this point, they are done with hydroxychloroquine, lopinavir-ritonavir, and interferon-β1a, but others, like monoclonal antibodies, have since been added (this is the adaptive trial design). The data available is an interim analysis after a total of 11,266 patients were randomized.
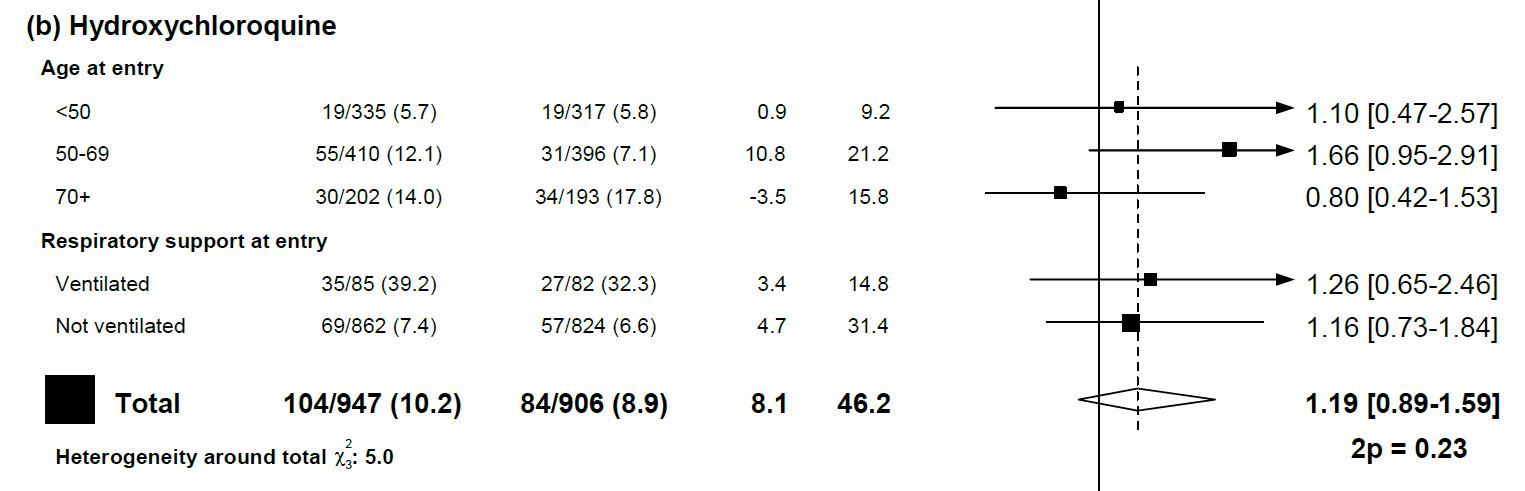
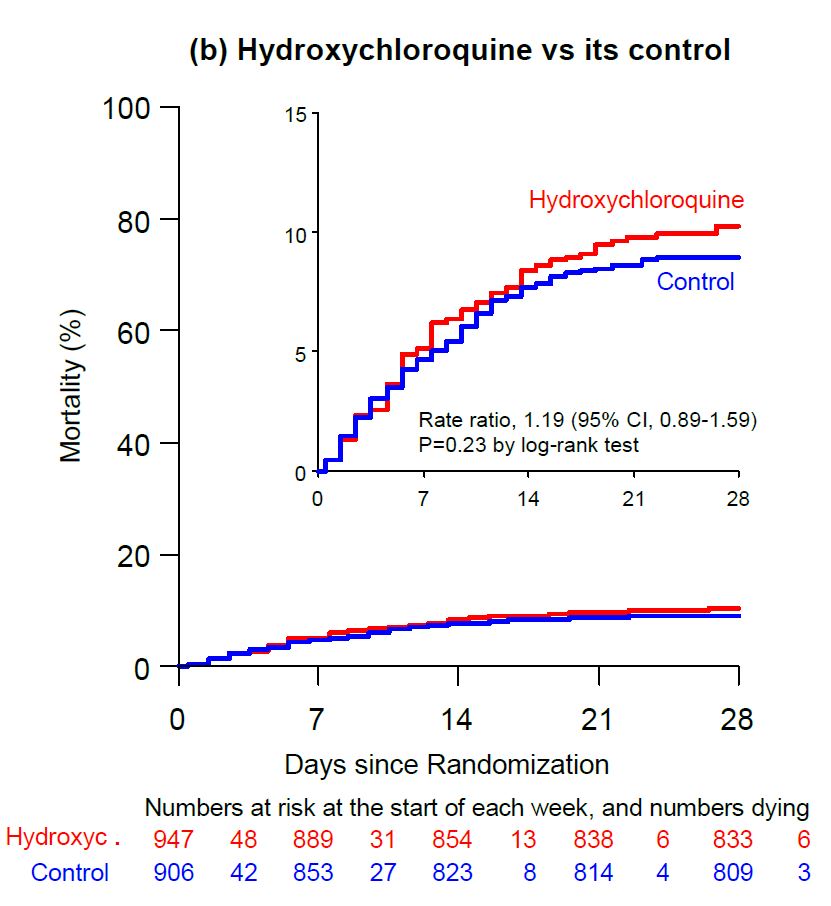
Focusing specifically on hydroxychloroquine, there were 947 patients randomized to treatment and 906 randomized to usual care. (This is not placebo controlled data, which does increase the risk of bias.) Hydroxychloroquine was prescribed with a loading dose of 800mg at 0 and 6 hours, and then 400mg orally twice a day for 10 days. Mortality was not improved with hydroxychloroquine, with the point estimate actually being on the side of harm (11% vs 9%, RR 1.19, 95% CI 0.89-1.59.) There was no difference in need for ventilation and hydroxychloroquine actually increased the risk of being hospitalized at 7 days (64% vs 54%).
Obviously those numbers are not great, but it is the meta-analysis that is truly damning. There are 29 trials looking at hydroxychloroquine for COVID-19. Combined, the relative risk of mortality is 1.10 with a 95% confidence interval from 0.99 to 1.22. Although that doesn’t prove harm, it clearly eliminates any possibility of benefit, and makes increased mortality the most likely outcome.
That meta-analysis includes a lot of small and imperfect trials. There really have only be 2 large, well-done RCTs of hydroxychloroquine: SOLIDARITY and RECOVERY. (RECOVERY 2020) If you only look at those two trials, the results are the same, with a RR of 1.11 (95% CI 0.99-1.24)
So hydroxychloroquine is probably killing patients. The medical profession, in our overzealous need to do something, was probably killing patients. If the mortality rate in COVID-19 is improving with time, it might simply be because we are prescribing fewer unproven, unnecessary, and potentially harmful chemicals.
It would be tempting to treat hydroxychloroquine as an outlier. After all, it should have been obvious that it didn’t work the moment that it was endorsed by Trump. However, I think this is a very important cautionary tale. There are still many treatments being used for COVID-19 that have absolutely no evidence of benefit.
But this isn’t a COVID specific problem. We have a long history in medicine of adopting interventions long before there is adequate (or even any) evidence. Optimism is good, but naive optimism in the clinical realm can result in significant harm to our patients.
We have never proven a benefit for thrombolytics in stroke, but we continue to blindly throw them at patients. Many jumped on ‘metabolic resuscitation’ of sepsis without any good evidence. We use epinephrine in cardiac arrest. We use PPIs in undifferentiated GI bleeds. We even prescribe medications that have been shown to be harmful, like heparin in NSTEMIs.
Essentially everything we do causes harm, even if the harm is just from lost opportunity cost. Our baseline must be to assume that novel interventions cause harm. From that baseline, it becomes clear that we cannot adopt new treatments until there is reasonable evidence of benefit.
Of course, don’t prescribe hydroxychloroquine for COVID patients. More importantly, let the hydroxychloroquine fiasco be a cautionary tale. How many of the treatments you currently prescribe lack adequate evidence and might be hurting your patients?
References
Carley S, Horner D, Body R, Mackway-Jones K. Evidence-based medicine and COVID-19: what to believe and when to change. Emerg Med J. 2020;emermed-2020-210098. doi:10.1136/emermed-2020-210098 PMID: 32651176
Pan H, Peto R, Karim QA, et al. Repurposed antiviral drugs for COVID-19; interim WHO SOLIDARITY trial results. medRxiv. Published online October 15, 2020:2020.10.15.20209817. doi:10.1101/2020.10.15.20209817 Published as a preprint: https://www.medrxiv.org/content/10.1101/2020.10.15.20209817v1
RECOVERY Collaborative Group, Horby P, Mafham M, Linsell L, Bell JL, Staplin N, Emberson JR, Wiselka M, Ustianowski A, Elmahi E, Prudon B, Whitehouse T, Felton T, Williams J, Faccenda J, Underwood J, Baillie JK, Chappell LC, Faust SN, Jaki T, Jeffery K, Lim WS, Montgomery A, Rowan K, Tarning J, Watson JA, White NJ, Juszczak E, Haynes R, Landray MJ. Effect of Hydroxychloroquine in Hospitalized Patients with Covid-19. N Engl J Med. 2020 Oct 8. doi: 10.1056/NEJMoa2022926. Epub ahead of print. PMID: 33031652.



7 thoughts on “Hydroxychloroquine: A tale of overzealous optimism and patient harm”
Hi Justin, thank you for all that you do, but why are you referencing retracted papers?
Solidarity was the fraudulent one that faked its numbers, and was subsequently retracted by the Lancet. They gave 4 times the toxic doses of HCQ to patients in ICU – late in the course, with out screener and adjuncts, with other meds that increase QT.
Recovery study also used similar toxic doses.
fromthetrenchesworldreport.com/dr-meryl-nass-discovers-hydroxychloroquine-experiments-were-designed-to-kill-covid-patients-how-many
It is a bit of an honour to have the first conspiracy theory in the comments on this site.
SOLIDARITY has not been retracted – in fact, it hasn’t even been published yet. The article referenced is just the preprint, but the results are the results. The dose used is essentially the same dose used to treat malaria. There is no reason to think it is too high, nor is there any reason to think that hydroxychloroquine provides any value to COVID-19 patients. Whenever there are negative trials in medicine, we need to consider whether the right dose was used, but we almost certainly have enough evidence on hydroxychloroquine at this point to know that it doesn’t help and shouldn’t be used even in the context of further trials. There are more important things to do with our research dollars.
Thank you, it is interesting…I went back and this is the Lancet study that was recently retracted: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31180-6/fulltext?fbclid=IwAR3aXXhB2gKoDX8qiZbcrhXdv-CmcTeG36jlgxcRNmKkXyngJ320PW8hO2M . It is referred to as the SOLIDARITY trial in the first link and it sounds like the trial was subsequently resumed??
No – SOLIDARITY is a massive, World Health Organization organized randomized control trial. It is a high quality trial (although like all trials, imperfect). The retracted paper you are referring to was supposed to be an observational trial, but was fraudulent, as the authors had a database company they were apparently trying to sell. The conclusions about hydroxychloroquine have nothing to do with the retracted article, or really any of the observational data. What you need is RCTs, and we have 2 high quality RCTs that show hydroxychloroquine clearly doesn’t work, and is most likely harmful. The website you are linking to is clearly a fringe conspiracy theory website. I would stick to the primary medical literature if you want a sense of good medical science.
You are actually an idiot. the dosage was far higher in this trial than is normally dosed and so it is not surprising that the results are as you show. Hydroxychloroquine works and is absolutely efficacious in the early stages of the disease!!
Care to share any RCT data that shows that hydroxychloroquine is “absolutely efficacious in the early stages of the disease”? There isn’t any. All the studies have been covered on this blog, and everything available is consistent with hydroxychloroquine hurting people, or at very best not helping.
Of course, resorting to ad hominems and providing no evidence for your claims is a good headstart to a productive conversation, just as much as anecdotal evidence is surely the way to establish working treatments.
For the sake of humanity, I hope you’re not a practicing or working member of health services. If so, you might want to stop and rethink your oath : ”First do no harm”.